February 03, 2026
3 min read
Key takeaways:
- Adults receiving tirzepatide had greater improvement in PHQ-9 score than those receiving placebo.
- Suicidal ideation was reported by 0.6% of the tirzepatide group, with most events deemed low risk.
Once-weekly subcutaneous tirzepatide may not raise risk for depression compared with placebo, according to a post hoc analysis of the SURMOUNT trials.
As Healio previously reported, in January the FDA requested that risk for suicidal ideation and behaviors be removed from labels for liraglutide (Saxenda, Novo Nordisk), injectable semaglutide 2.4 mg (Wegovy, Novo Nordisk) and tirzepatide (Zepbound, Eli Lilly).

Data were derived from Wadden TA, et al. Obesity. 2026;doi:10.1002/oby.70122.
In data published in Obesity, researchers found adults receiving tirzepatide in three SURMOUNT trials did not experience worsening of depression throughout the studies.
“The low occurrence of these events with tirzepatide is similar to that observed in pooled analyses of semaglutide 2.4 mg and liraglutide 3 mg, both GLP-1 receptor agonists approved for weight management,” Thomas A. Wadden, PhD, professor of psychology in psychiatry at Perelman School of Medicine, University of Pennsylvania in Philadelphia, told Healio. “The present report provides the first detailed analysis of the risk of these psychiatric events with tirzepatide.”

Thomas A. Wadden
Researchers analyzed data from the SURMOUNT-1, SURMOUNT-2 and SURMOUNT-3 trials. In all three studies, adults with obesity or overweight with at least one weight-related comorbidity were randomly assigned to once-weekly subcutaneous tirzepatide or placebo for 72 weeks. Depression was assessed through the Patient Health Questionnaire-9 (PHQ-9). The Columbia-Suicide Severity Rating Scale was administered to assess suicidal ideation and behavior. Neuropsychiatric events were also collected during study visits.
Depression symptoms
There were 4,056 adults included in the analysis (63% women; 74% white), of whom 2,806 received tirzepatide and 1,250 received placebo. Mean PHQ-9 scores at baseline were 2.7 for the tirzepatide group and 2.6 for the placebo group, indicating minimal or no depression symptoms. At 72 weeks, adults receiving tirzepatide had a 0.6-point greater drop in PHQ-9 score than placebo.
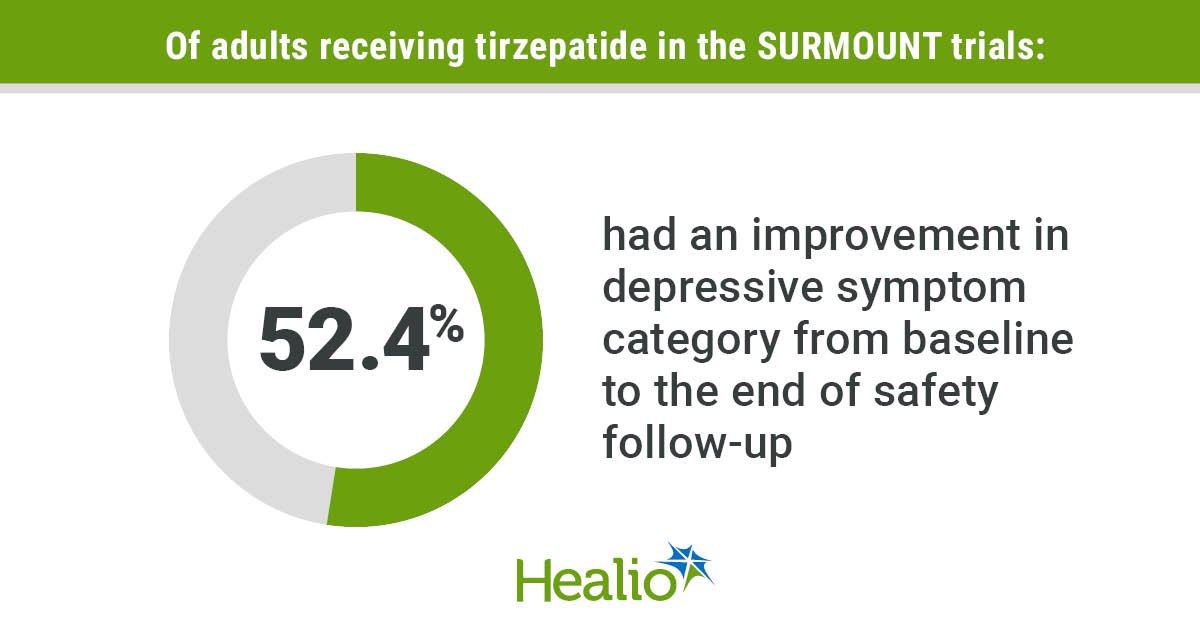
Of adults receiving tirzepatide who had no or minimal depression symptoms at baseline, 79.4% remained in that category through the end of safety follow-up, 17% reported mild depression symptoms, 2.9% had moderate symptoms, 0.7% reported moderately severe symptoms and 0.1% had severe symptoms. A lower proportion of adults receiving tirzepatide moved to a worsened depressive symptom category vs. those receiving placebo (18.2% vs. 24.3%; P < .001), and a higher percentage of the tirzepatide group moved to a less severe category for depressive symptoms compared with the placebo group (52.4% vs. 41.8%; P < .001).
Suicidal ideation and behaviors
At baseline, 70 participants receiving tirzepatide and 38 receiving placebo reported a history of suicidal ideation or behavior. Through the end of safety follow-up in each trial, 0.6% of adults in each of the tirzepatide and placebo groups reported suicidal ideation, with most of these reports deemed low risk. Of participants, 0.3% those receiving tirzepatide and 0.1% of the placebo group reported suicidal ideation deemed moderate risk. Three adults receiving tirzepatide and one receiving placebo had suicidal ideation deemed high risk.
Suicidal behavior was reported by two participants receiving tirzepatide and none receiving placebo.
At least one treatment-emergent nervous system disorder adverse event occurred in 15.8% of the tirzepatide group and 13% of the placebo group. There was no difference in the occurrence of treatment-emergent psychiatric disorders between the tirzepatide and placebo groups.
Assessing mental health
Wadden said he and colleagues supported the FDA’s decision to remove suicidal ideation and behavior risk from the labels of incretin-based obesity drugs, but health care professionals need to conduct mental health assessments for all patients with obesity.
“Persons with obesity, particularly with a BMI of more than 40 kg/m2, are at substantially increased risk of major depression and anxiety disorders,” Wadden said. “It’s critical that they receive the same mental health care that persons of average weight would when presenting with these conditions.”
Wadden said more studies need to be performed on the impact of incretin-based obesity drugs for people with adequately controlled psychiatric disorder.
“Randomized trials of the GLP-1 obesity medications largely excluded persons who, in the past 2 years, had experienced major depression, schizophrenia or bipolar disorder, or who had a lifetime history of suicide attempt,” Wadden said. “GLP-1 medications potentially could be beneficial to individuals who suffer from these conditions. Small, carefully controlled studies would appear warranted, as would a close examination of the FDA’s recent retrospective cohort study of more than 2 million individuals. The FDA’s dataset likely included a far greater range of psychiatric status than found in the randomized controlled trials that evaluated tirzepatide and semaglutide for chronic weight management.”
For more information:
Thomas A. Wadden, PhD, can be reached at wadden@pennmedicine.upenn.edu.
Sources/Disclosures
Source:
Wadden TA, et al. Obesity. 2026;doi:10.1002/oby.70122.
Disclosures:
Wadden reports advising for Novo Nordisk and WW and receiving grants on behalf of University of Pennsylvania from Eli Lilly, Epitomee Medical and Novo Nordisk. Please see the study for all other authors’ relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<








Leave a Reply