April 17, 2026
3 min read
Key takeaways:
- Patients with very severe hidradenitis suppurativa often reach an efficacy ceiling with monotherapy.
- Adding a JAK1 inhibitor, anti-tumor necrosis factor inhibitor or anti-interleukin could improve outcomes.
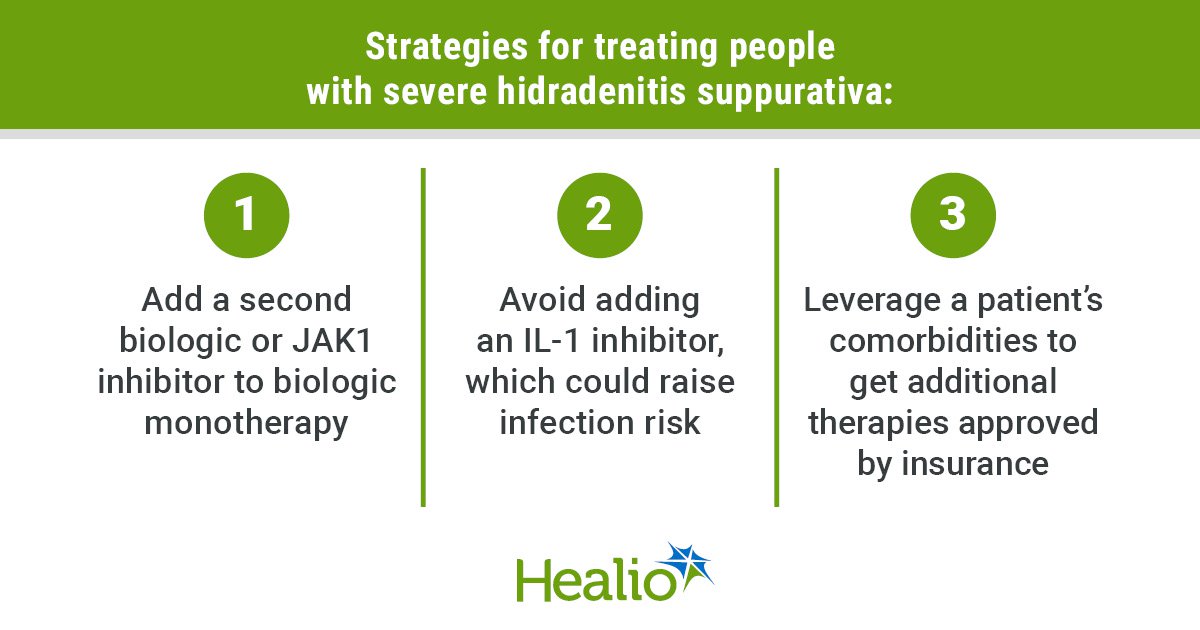
DENVER — Dual biologic therapy should be considered for patients with very severe hidradenitis suppurativa, according to a speaker at the American Academy of Dermatology Annual Meeting. However, caution is advised for some combinations.
Medications and procedures that may improve HS signs and symptoms are “not quite enough” for some patients, Jennifer L. Hsiao, MD, FAAD, associate professor of dermatology at Keck School of Medicine at the University of Southern California and a member of Healio Dermatology’s Peer Perspective Board, said during a presentation.

Data derived from Hsiao J. HS: Dual biologics and biologic + SMI. Presented at: American Academy of Dermatology Annual Meeting; March 27-31, 2026; Denver.
“Every time you start a monotherapy biologic agent and give it an appropriate time to work, you keep running into an efficacy ceiling,” Hsiao said. “Every time you get halfway up that mountain, the patient is feeling better, but they are still not functional. They can’t go about their day-to-day [routine] and they are still on many pain medications. When this happens, instead of using prednisone and antibiotics … I’d rather add a second targeted therapy.”

Jennifer L. Hsiao
There are currently three FDA-approved biologics for HS: adalimumab (Humira, AbbVie), a tumor necrosis factor (TNF) inhibitor; secukinumab (Cosentyx, Novartis), an interleukin-17A inhibitor; and bimekizumab (Bimzelx, UCB), an IL-17A/F inhibitor. Due to the limited approved options, Hsiao said physicians also use JAK inhibitors and other IL inhibitors, such as IL-23 and IL-12/23, off-label.
Hsiao recommends the following dual biologic therapies for patients with very severe HS:
- an anti-TNF as a base plus an anti-IL-17, anti-IL-23 (or 12/23) or a JAK1 inhibitor;
- an anti-IL17 as a base plus an anti-TNF, anti-IL-23 (or 12/23) or a JAK1 inhibitor; or
- a JAK1 inhibitor as a base plus an anti-TNF, anti-IL-17 or anti-IL-23 or anti-IL-12/23.
Combining these medications for HS is not a well-researched practice, but other specialties have been doing it for years, according to Hsiao.
“Our gastroenterology and rheumatology colleagues have been using combination therapies to treat their patients with intestinal bowel disease,” Hsiao said. “So, I think it is helpful to look at their literature to see how efficacy and safety have gone for them.”
Safety considerations
In a phase 2a study published in January 2022 in the Journal of Crohn’s and Colitis, approximately 70 participants each were assigned to receive golimumab (Simponi, Johnson & Johnson), guselkumab (Tremfya, Johnson & Johnson) or a combination of the two. At week 12, the combination group achieved higher efficacy with the same adverse events rate compared with the monotherapy arms. Over 36% of participants in the combination group achieved clinical remission vs. 22.2% and 21.1% in the golimumab and guselkumab arms, respectively. Adverse events that led to discontinuation occurred in 2.8% of the combination group, 4.2% of the golimumab group and 1.4% of the guselkumab group.
Similarly, a phase 2 trial published in Arthritis & Rheumatology showed no increased risk for serious adverse events in patients with psoriatic arthritis who were assigned an anti-TNF and anti-IL-17A combination vs. those who received anti-TNF monotherapy.
Although dual biologic therapy may be promising for HS, Hsiao warns against a particular combination: TNF inhibitors plus anti-IL-1s.
“In a rheumatoid arthritis study that evaluated etanercept (Enbrel, Amgen), a TNF-inhibitor, vs. etanercept plus anakinra (Kineret, Sobi), an anti-IL-1, there was an increased risk for serious infection seen [with combination therapy],” Hsiao said. “In my personal practice, I do not combine anti-TNFs and anti-IL-1s because, in part, it would be harder to explain the decision to a patient if they did end up getting a serious infection and this was in the literature.”
Navigating insurance hurdles
When dual biologic therapy is deemed necessary, insurance coverage for the second agent requires strategic planning, Hsiao said. One of the best approaches is to leverage a patient’s comorbidities, according to Hsiao.
“For example, if I have a biologic for HS, I can get the JAK inhibitor covered for concomitant atopic dermatitis,” Hsiao said.
Hsiao noted that insurance coverage may also be easier if one infusion plus one subcutaneous injectable is prescribed vs. two subcutaneous injectables.
Other considerations before prescribing dual biologics, according to Hsiao, include planning ahead with the Shingrix zoster vaccine (GlaxoSmithKline) if introducing a JAK1 inhibitor, conducting lab monitoring depending on the biologic used, documenting a patient’s disease baseline on monotherapy prior to combination treatment initiation and asking the patient what their administration preference is.
“My hope is that when we see a patient with HS who comes to our clinic, that regardless of their severity level, we feel a level of comfort in treating them,” Hsiao said.
Sources/Disclosures
Source:
Hsiao J. HS: Dual biologics and biologic + SMI. Presented at: American Academy of Dermatology Annual Meeting; March 27-31, 2026; Denver.
References:
Disclosures:
Hsiao reports receiving consultant fees, speaking fees, grants or research funding from Aclaris Therapeutics, Amgen, AstraZeneca, Boehringer Ingelheim, Galderma, Insmed, Leo Pharma, MoonLake Immunotherapeutics, Navigator Medicines, Novartis, Oruka Therapeutics, Pfizer, Sanofi and UCB.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<












Leave a Reply