January 30, 2026
5 min read
Key takeaways:
- Participants were aged 70 years and older with moderate hearing impairment and no dementia.
- Estimated mean cognition scores for participants with and without hearing aid prescriptions at 7 years were similar.
Hearing aids did not lead to any significant differences in cognitive testing among older patients with moderate hearing loss, but these devices may reduce risks for dementia, according to data published in Neurology.
Residual confounding may explain these findings, Lachlan Cribb, BSci, MEpi, a PhD student at the School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia, and colleagues wrote.

Data derived from Cribb L, et al. Neurology. 2026;doi:10.1212/WNL.0000000000214572.
“Hearing loss has been linked to a greater risk of developing dementia. But it was not known whether using a hearing aid could help reduce that risk,” Cribb told Healio.
The 2023 randomized Aging and Cognitive Health Evaluation in Elders (ACHIEVE) trial compared a hearing aid intervention with health education among older adults in the United States with hearing loss.
“They found little overall benefit of hearing aids for slowing cognitive decline over 3 years, though there was a benefit in a subgroup with elevated baseline risk,” Cribb said.
“Due to its relatively short follow-up, diagnosed dementia was not examined,” he continued. “The goal of our study was to investigate the effects of hearing aids on dementia and cognition over a period of 7 years.”
The study examined data from patients aged 70 years and older with moderate hearing impairment but no dementia. All patients were enrolled in the ASPirin in Reducing Events in the Elderly (ASPREE) randomized, placebo-controlled trial and its ASPREE-eXTension follow-up.
The cohort included a median of 664 patients (mean age, 75.1 years; 49% women; 98% white) who received a prescription for a new hearing aid in the previous 3 years, including 402 who always or often used their hearing aid and 188 who sometimes or rarely used it, and a median of 2,113 (mean age, 74.2 years; 48% women; 99% white) who did not.
At 7 years, the subgroup with prescriptions included 51 deaths, 25 cases of dementia and 131 cases of cognitive impairment, and the subgroup with no prescriptions included 123 deaths, 92 cases of dementia and 411 cases of cognitive impairment.
“After carefully adjusting for a range of lifestyle and health factors that differed across participants, we found that participants with hearing loss who were prescribed hearing aids had a similar rate of cognitive change over 7 years to those who were not prescribed hearing aids,” Cribb said.
Estimated mean scores across four cognitive tests at 7 years for these subgroups had a mean difference of 0.03 standard deviation [SD] (95% CI, –0.14-0.21), the researchers said, and the estimated mean scores for those who often or always used hearing aids were similar to the scores for those who never used hearing aids as well (mean difference = 0.02 SD; 95% CI, –0.19-0.23).
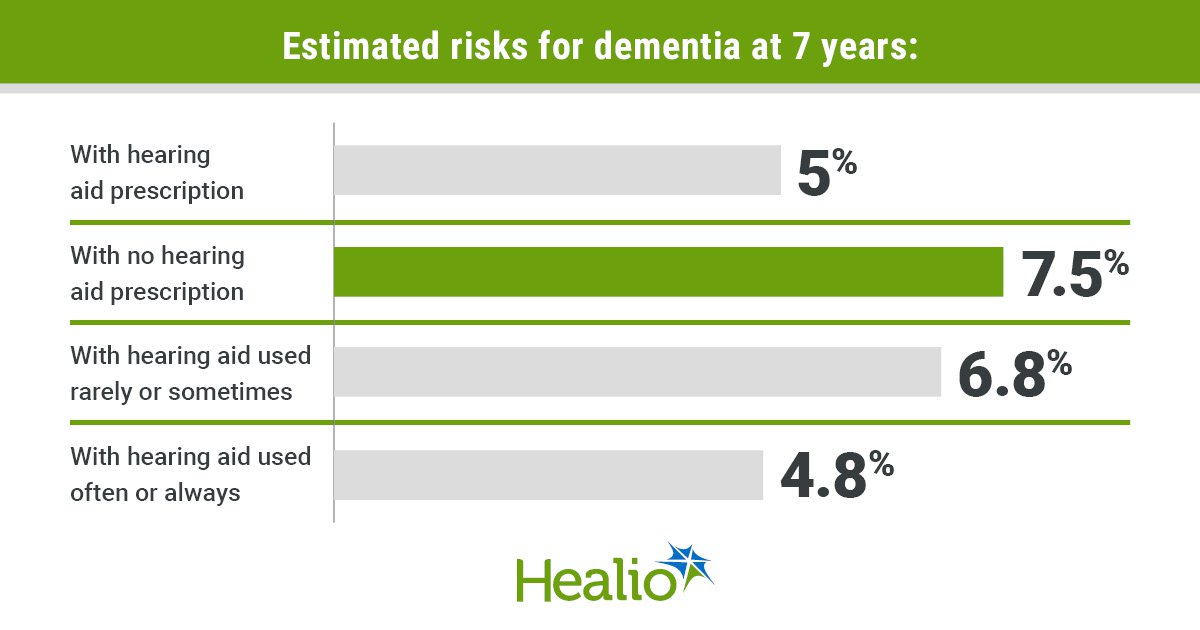
Estimated risks for dementia at 7 years included 5% for those with a prescription for a hearing aid and 7.5% for those with no prescription (RR = 0.67; 95% CI, 0.37-0.97).
“Those who were prescribed hearing aids had a 33% lower risk of diagnosed dementia, with the degree of risk reduction proportional to how frequently participants reported using their hearing aid,” Cribb said.
Specifically, these risks included 7.3% for those who never used a hearing aid, 6.8% with rare or sometimes use and 4.8% for those who used a hearing aid often or always.
The risk ratio for dementia was 0.67 (95% CI, 0.29-1.06) among those who used a hearing aid often or always compared with those who never used one.
Estimated risks for cognitive impairment at 7 years included 36.1% for those with a prescription for a hearing aid and 42.4% for those with no prescription (RR = 0.85; 95% CI, 0.7-1), or a 15% lower risk with a prescription.
Specific risks included 41.5% for those who never used a hearing aid, 39.2% for those with rare or sometimes use and 35.7% for those who often or always used a hearing aid.
The risk ratio for cognitive impairment among patients who often or always used a hearing aid was 0.86 (95% CI, 0.66-1.06) compared with those who never used one.
Further, mean differences in overall cognition scores at 7 years were greater for patients with an overall baseline Modified Min-Mental State Examination score less than 95 (0.17 SD; 95% CI, –0.07-0.4) and baseline better-ear four-frequency pure tone average of 30 dbHL or higher (0.12 SD; 95% CI, –0.12-0.36).
As a sensitivity analysis, the researchers compared the estimated 3-year mean differences in overall cognition scores between patients who often or always used hearing aids and those who never used them with the effect estimate from the ACHIEVE trial. These were 0.04 standard deviations (95% CI, –0.05-0.13) and 0 standard deviations (95% CI, –0.08-0.08), respectively, which the researchers called similar.
Further, the estimated 7-year mean difference in overall cognition scores between those patients with a prescription and those with no prescription was greater (0.14 SD; 95% CI, –0.08-0.35) when multiply imputed audiometry data were used to define the eligibility criterion of moderate hearing loss. Overall risks for dementia and cognitive impairment were considerably greater when audiometry was used to define the eligible sample.
Based on these findings, the researchers said that prescriptions for hearing aids did not lead to any substantial changes in overall cognition scores for older patients with moderate hearing impairment.
“We were surprised to find evidence of reduced dementia risk without a corresponding reduction in overall age-related cognitive change,” Cribb said.
“We postulate that this could be due to the good cognitive health of our sample at baseline (reducing scope for treatment benefit) and/or to the complexity of age-related cognitive change, which is influenced by a diverse range of lifestyle and health factors,” he continued.
The researchers said these findings may be due to possible links between sensory loss and dementia risk. As neuronal activity altered by hearing loss may exacerbate existing pathology in Alzheimer’s disease, they said, amplification may delay or prevent dementia onset for these patients but have less benefit for patients who do not have this pathology.
They added that the findings may support the hypothesis that hearing loss causes sensory deprivation, impacting regional brain volume.
Cribb and colleagues called for long-term randomized trials and observational studies in populations who are at a high risk for cognitive decline. Overall, Cribb said, the use of hearing aids to treat hearing loss could reduce risks for dementia in a dose-dependent manner.
“We found that treating hearing loss with hearing aids could reduce dementia risk in a dose-dependent manner,” he said.
“While we can’t conclude that hearing aids cause a reduction in dementia, together with the findings of ACHIEVE, this suggests that screening and treatment for hearing loss may be a low-risk and cost-effective way of reducing dementia risk,” he added.
“This may be especially true for individuals with risk factors for cognitive impairment, including preexisting cognitive difficulties, limited education, and cardiovascular and metabolic comorbidities.”
Perspective
Back to Top

Meher Lad, MBBS, PhD
Newcastle upon Tyne Hospitals NHS Foundation Trust
Disclosures: Lad reports no relevant financial disclosures.
Perspective
Back to Top

Willa Brenowitz, PhD, MPH
Kaiser Permanente Northwest Center for Health Research
Disclosures: Brenowitz reports no relevant financial disclosures.
Sources/Disclosures
Source:
Cribb L, et al. Neurology. 2026;doi:10.1212/WNL.0000000000214572.
References:
For more information:
Lachlan Cribb, BSci, MEpi, can be reached at allergy@healio.com.
Disclosures:
Cribb reports no relevant financial disclosures. See the study for the other authors’ relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<






Leave a Reply