April 22, 2026
2 min read
Key takeaways:
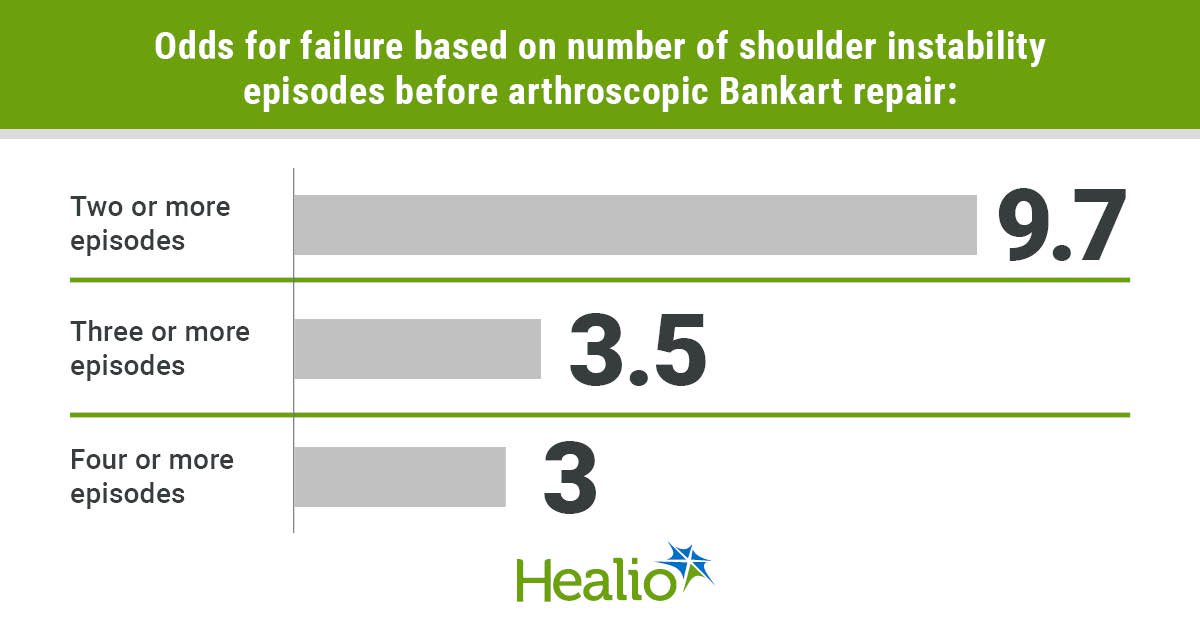
- Two or more shoulder instability episodes had 9.7 times increase in odds for failure vs. one instability episode.
- A threshold of two or more shoulder instability episodes had an area under the curve of 0.72.
NEW ORLEANS — Patients with two or more shoulder instability episodes before arthroscopic Bankart repair had a significant increase in risk for recurrent instability postoperatively, according to results presented here.
“When a patient has one preoperative instability episode, considering surgery would help them have a better outcome,” Ryan T. Lin, BS, first author of the study and third year medical student at the University of Pittsburgh School of Medicine, told Healio about results presented at the American Academy of Orthopaedic Surgeons Annual Meeting Specialty Day. “Once they have two or more instability episodes, we know that they are going to have a higher risk for failure. Earlier surgical management, or at least earlier evaluation of surgical management, in these young patients typically has the best outcomes.”

Data derived from Gilbert R, et al. Paper 4. Presented at: American Academy of Orthopaedic Surgeons Annual Meeting Specialty Day; March 6, 2026; New Orleans.
Lin, along with Ryan Gilbert, BA, also of the University of Pittsburgh School of Medicine, and colleagues, retrospectively reviewed data from 151 patients with on track Hill-Sachs lesions who underwent primary isolated arthroscopic Bankart repair for anterior shoulder instability between 2007 and 2019.
“In this study, we defined postoperative failure as some recurrent instability after the procedure that could take the form of frank dislocation requiring reduction or a perception of instability and subluxation,” Gilbert said in his presentation.
Gilbert said recurrent instability occurred in 28 patients for an overall failure rate of 19%, with a variation in failure rate based on the number of preoperative instability episodes.
In a multivariable regression model, controlling for age and distance to dislocation, Gilbert said two or more preoperative instability episodes had 9.7 times increase in odds for failure vs. one instability episode. Patients with three or more instability episodes had 3.5 times the odds for failure vs. two or more episodes, and patients with four or more instability episodes had three times the odds for failure compared with three or fewer instability episodes.
“Once you got up to five or more, there was not a significantly greater increase in odds compared with if you had four or fewer episodes,” Gilbert said. “But the steepest increase happens between two episodes vs. one episode.”
Gilbert said receiver operator curve analysis showed a threshold of two or more preoperative instability episodes vs. one episode had an area under the curve of 0.72, a sensitivity of 89 and a specificity of 55% for recurrent instability.
“We tried other thresholds like three or more episodes or four or more episodes, and all of those gave us lower areas under the curve, which, altogether, indicates that two or more is that threshold that best predicts failure after arthroscopic Bankart repair,” Gilbert said.
Finally, patients who exceeded the threshold of two or more preoperative instability episodes had a greater percentage of glenoid bone loss, larger Hill-Sachs lesions, smaller dislocation and a greater proportion of near-track status for Hill-Sachs lesion, according to Gilbert.
When treating athletes with shoulder instability, Lin told Healio there are a number of variables to take into consideration, including whether the patient is undergoing recruitment.
He said these results provide evidence that performing surgical stabilization after one shoulder instability event may be “the best optimal management of treatment. That can be part of the conversation for the surgeon to tell the family about their outcomes, and that could be something that can, hopefully, change patient management.”
For more information:
Ryan Gilbert, BA, can be contacted at gilbertr6@upmc.edu.
Ryan T. Lin, BS, can be contacted at linr5@upmc.edu.
Sources/Disclosures
Source:
Gilbert R, et al. Paper 4. Presented at: American Academy of Orthopaedic Surgeons Annual Meeting Specialty Day; March 6, 2026; New Orleans.
Disclosures:
Gilbert and Lin report no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<












Leave a Reply