April 28, 2026
3 min read
Key takeaways:
- Asian American and Native Hawaiian Islanders lack care for conditions that disproportionally affect them.
- Some expressed fears of losing insurance or being detained or deported when accessing care.
SAN FRANCISCO — There are substantial gaps in access to care and screening for conditions like hepatitis B, diabetes and tuberculosis among Asian American, Native Hawaiian and Pacific Islander communities, a nationwide survey shows.
According to Rita K. Kuwahara, MD, MIH, FACP, Asian American, Native Hawaiian and Pacific Islander (AA and NH/PI) communities are disproportionally impacted by these chronic diseases.

Data derived from Kuwahara R. Closing the health equity gap: Opportunities to address Asian American, Native Hawaiian and Pacific Islander health. Presented at: ACP Internal Medicine Meeting; April 16-18, 2026; San Francisco.
For example, “about one in 12 AA and NH/PI adults have chronic hepatitis B, according to the CDC, and over half of AA adults with diabetes remain undiagnosed,” Kuwahara, a primary care internal medicine physician and Healio Primary Care Peer Perspective Board member, said at ACP’s Internal Medicine Meeting.
She told Healio that she conducted a survey to assess opportunities in the clinical setting to improve the diagnosis and treatment of these diseases among AA and NH/PI communities living in the U.S. “and examine how U.S. health and immigration policy changes affect access to care.”
Kuwahara surveyed 1,027 AA and NH/PI adults (51% women) on their past screenings for diabetes, tuberculous and HBV, as well as delays or absences of care and the reasons for such.
The nationwide survey was conducted electronically in September 2025, and the data were weighted by age, sex, education, census region, U.S. born and Asian origin/ethnicity.
Of all the surveyed participants, 90% had a primary care physician, but only 24% of those with no health insurance had a primary care physician.
Kuwahara found that among participants aged 35 to 70 years, only 58% of those with a BMI between 23 kg/m2 to 24.9 kg/m2 were previously screened for diabetes, “despite the fact that Asian Americans should be classified as being overweight starting at a BMI of 23 kg/m2, instead of 25 kg/m2, according to the U.S. Preventive Services Task Force, and should be screened for diabetes starting at a BMI of 23 kg/m2.”
She also found that 72% of surveyed participants aged 35 to 70 years with a BMI of 25 kg/m2 or higher were screened for diabetes.
Half of participants reported having previously been screened for tuberculous.
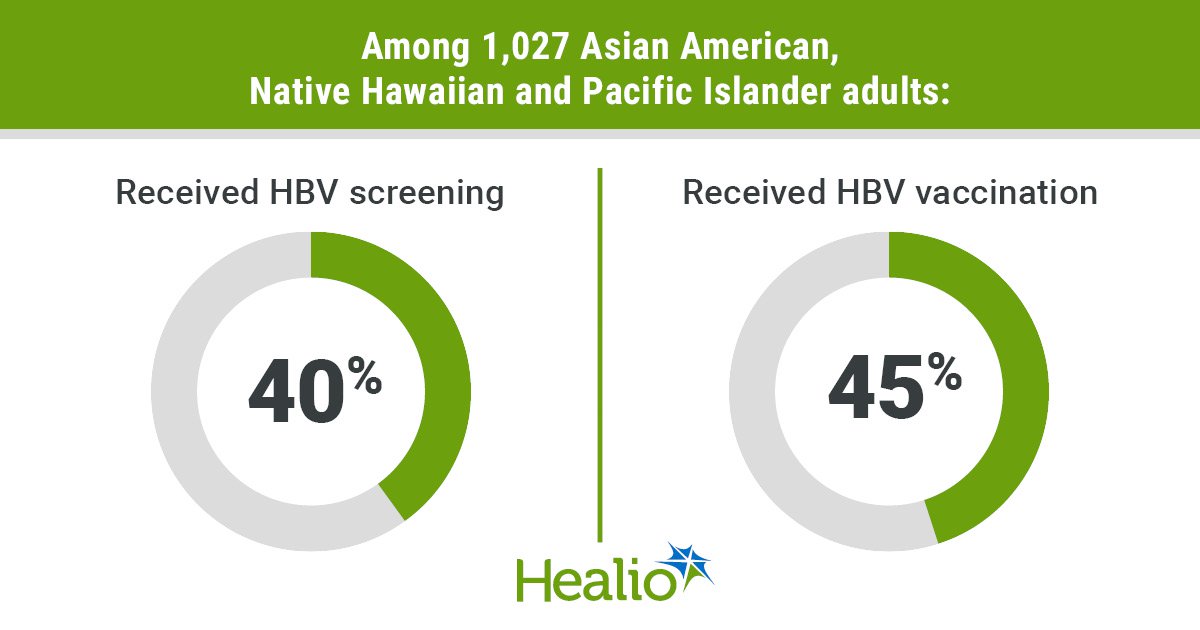
Kuwahara also found that 40% of surveyed adults were screened for HBV and 45% received the HBV vaccine.
Of adults diagnosed with chronic HBV:
- 75% saw a clinician at least yearly for HBV;
- 55% received follow-up education on HBV; and
- 35% received screening for liver cancer.
Kuwahara additionally reported that 15% of all surveyed adults, 24% of Affordable Care Act enrollees, 30% of Medicaid enrollees and 57% of those with no health insurance delayed or did not seek care due to cost.
Nearly half (48%) of surveyed Medicaid enrollees said they were afraid of losing their health insurance within the next year, as were 39% of Affordable Care Act enrollees.
Among non-U.S. citizens, 21% were afraid to seek care due to their fear of being detained or deported, while 13% were afraid to seek care out of fear it could affect their immigration status.
But Kuwahara added that 7% and 6% of U.S. citizens were also afraid of seeking care due to fears of being detained or deported or it affecting their immigration status, respectively, “so, this is not just an issue for non-U.S. citizens. These policies have created a broader chilling effect making individuals afraid to seek necessary health care in the U.S.”
Kuwahara told Healio that from a clinical perspective, “there are a few simple steps clinicians can take in the clinic to improve AA and NH/PI health. Findings from the survey indicate that clinicians should be screening all adults for HBV using the triple panel [Hepatitis B Surface Antigen, Hepatitis B Surface Antibody, Hepatitis B Core Antibody Total], which is already recommended by the CDC. We should be administering the HBV vaccine to all newborns, children and adults, and ensure that everyone who is diagnosed with chronic HBV is appropriately linked to follow-up care for hepatitis B.”
“This project is of value to internal medicine because it’s vital for internists to know if patients have undiagnosed chronic or infectious diseases, and internists should be aware of AA and NH/PI-specific clinical screening and prevention recommendations,” Kuwahara said.
She acknowledged that the survey data were self-reported, and “since the surveyed participants had a higher socioeconomic status than the general population, with nearly half (48%) reporting an annual household income of more than $100,000, the data presented here might be an underestimate of the true problem.”
Moving forward, there is a need to develop systems and practices to routinely screen AA and NH/PI populations for diseases disproportionately affecting the communities, including diabetes, HBV and tuberculosis, Kuwahara concluded, while PCPs “must be responsive to the changing U.S. health and immigration policies to protect and support patients afraid to access care due to immigration or financial concerns.”
For more information:
Rita K. Kuwahara, MD, MIH, FACP, can be reached at primarycare@healio.com.
Sources/Disclosures
Source:
Kuwahara R. Closing the health equity gap: Opportunities to address Asian American, Native Hawaiian and Pacific Islander health. Presented at: ACP Internal Medicine Meeting; April 16-18, 2026; San Francisco.
Disclosures:
Kuwahara reports no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<










Leave a Reply