Key takeaways:
- Ursodeoxycholic acid did not reduce complications with intrahepatic cholestasis of pregnancy.
- Its use was linked to higher rates of preterm and emergency cesarian deliveries.
CHICAGO — Ursodeoxycholic acid did not appear to improve maternal or fetal outcomes among patients with intrahepatic cholestasis of pregnancy, according to a retrospective cohort study presented at Digestive Disease Week.
The therapy also was associated with an increase in preterm and emergency cesarean deliveries.

Data derived from Rodrigues MD, et al. Maternal and fetal outcomes of intrahepatic cholestasis of pregnancy: Outcomes in a national matched cohort. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago.
Among patients with intrahepatic cholestasis of pregnancy, bile acid concentration is a key risk determinant for maternal and fetal morbidity.
“Intrahepatic cholestasis of pregnancy is a very challenging condition, and its management is driven by fetal risks,” Medora D. Rodrigues, MD, internal medicine physician and hospitalist at The Ohio State University Wexner Medical Center, told Healio. “[Ursodeoxycholic acid (UDCA)] has not shown a consistent benefit in improving perinatal outcomes, so the gap between its routine use and uncertain efficacy prompted us to evaluate real-world outcomes across all bile acid levels.”
Rodrigues and colleagues gathered data on adults with intrahepatic cholestasis of pregnancy from the TriNetX research network between 2006 and 2025, categorizing them by peak bile acid levels — less than 10 mol/L, 10 to 100 mol/L or greater than 100 mol/L.
Individuals included in analysis were matched by demographics, comorbidities and pregnancy-related risk factors and split into two cohorts — one that received UDCA and one that did not (n = 4,935 each).
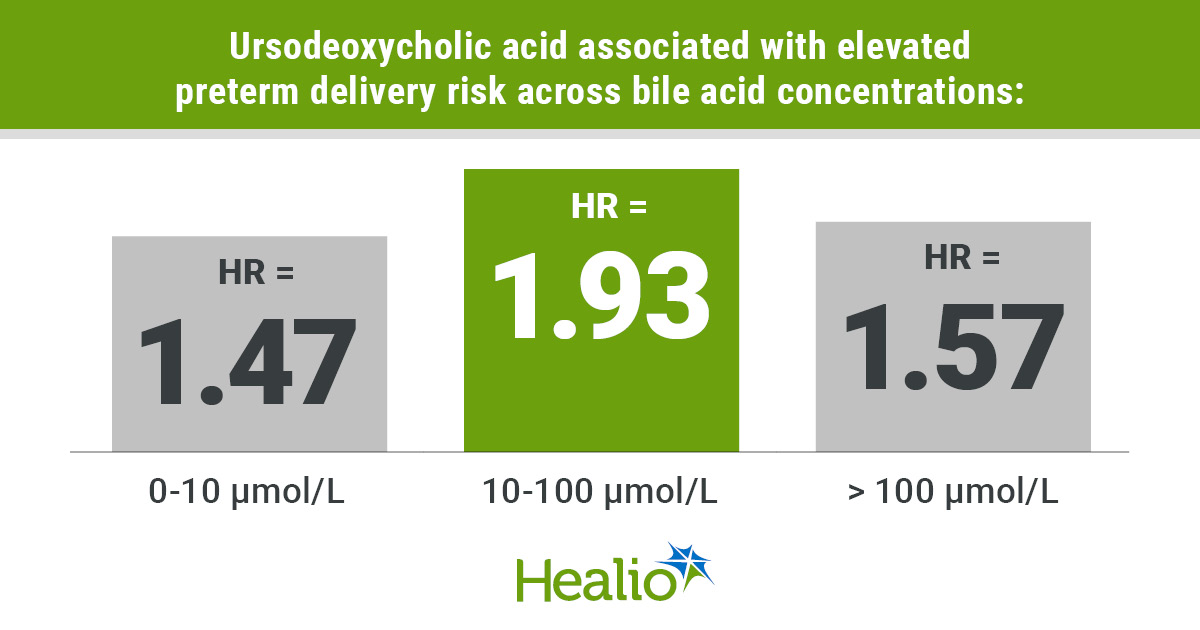
Results showed UDCA therapy was associated with elevated rates of preterm delivery regardless of bile acid concentration (< 10 mol/L: HR = 1.47; 95% CI, 1.09-1.99; 10-100 mol/L: HR = 1.93; 95% CI, 1.65-2.25; and > 100 mol/L; HR = 1.57; 95% CI, 1.05-2.35).
Individuals with bile acid levels up to 100 mol/L who received UDCA also were at significantly higher risk for emergency cesarean deliveries (< 10 mol/L: HR = 1.47; 95% CI, 1.04-2.09; 10-100 mol/L: HR = 1.28; 95% CI, 1.08-1.52).
Researchers found that UDCA had no impact on adverse fetal outcomes, growth restriction or maternal outcomes, including acute kidney injury and respiratory failure needing ventilation.
Given these findings, gastroenterologists should “be cautious about overstating the benefits of UDCA beyond pruritus relief,” Rodrigues said.
She also noted several aspects of the TriNetX dataset that limited the study.
“The exact timing, dosing and adherence to treatment were difficult to assess because the data are very granular, and the only thing we were able to evaluate was prescription fill by the patients,” she said.
Rodrigues emphasized the need for further research on this topic, particularly on mechanism-driven therapies, and for risk stratification for intrahepatic cholestasis of pregnancy based on patients’ bile acid levels.
For more information:
Medora D. Rodrigues, MD, can be reached at gastroenterology@healio.com.
Sources/Disclosures
Source:
Rodrigues MD, et al. Maternal and fetal outcomes of intrahepatic cholestasis of pregnancy: Outcomes in a national matched cohort. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago.
Disclosures:
Rodrigues reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<






Leave a Reply