April 17, 2026
6 min read
Key takeaways:
- ACP issued new guidance on breast cancer screening frequency and technique in women at average risk.
- The guidance is meant to reconcile differences in recommendations across medical groups.
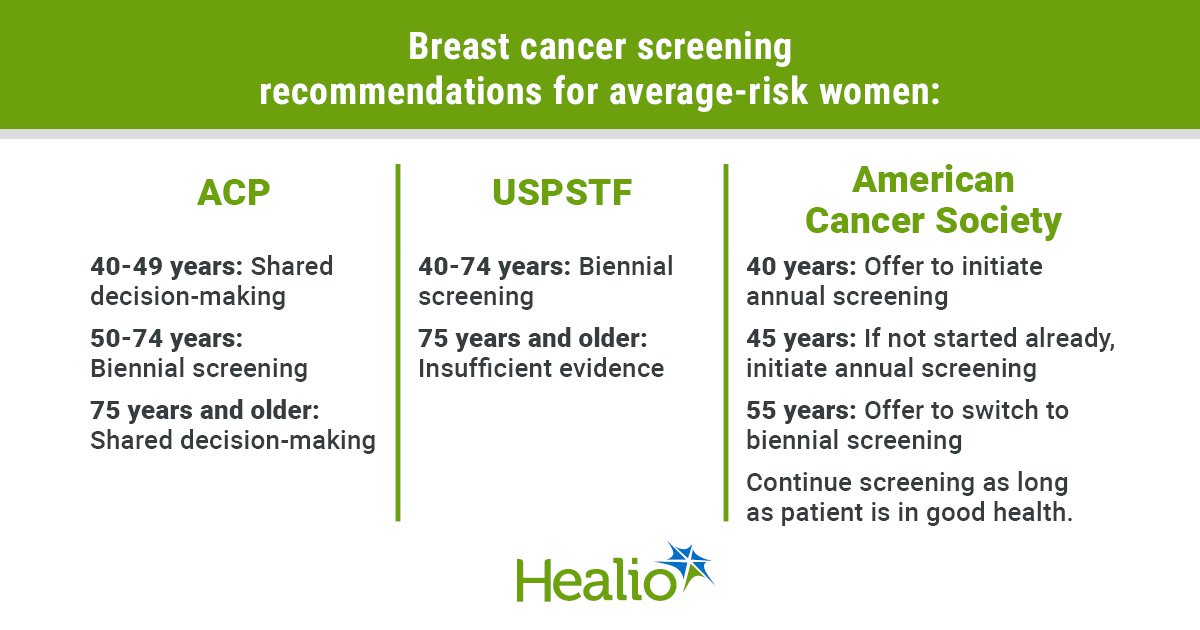
SAN FRANCISCO — All asymptomatic women aged 50 to 74 years at an average risk for breast cancer should receive biennial screening mammography, new ACP guidance published in Annals of Internal Medicine states.
Carolyn J. Crandall, MD, MS, MACP, chair of the ACP Guidelines Committee and a professor of medicine at David Geffen School of Medicine at the University of California, Los Angeles, unveiled the new guidelines during the plenary session at the ACP Internal Medicine Meeting.

“We considered the benefits, harms, patient preferences and values, and costs, and developed our guidance statements to help clinicians provide the best evidence-based care they can for their patients,” she told Healio. “ACP is a strong proponent of appropriate screening for breast cancer.”
The ACP guidelines conclude that the benefits of biennial screening outweigh the harms in this population, while annual screening “would create additional patient burden and costs, and does not provide clear evidence of added benefit over biennial screening,” Crandall and colleagues wrote.
Biennial screening could be started earlier in certain asymptomatic, average-risk women aged 40 to 49 years. The decision should be based on a discussion with the patient about their risk for breast cancer, their values and preferences, and the benefits and harms of screening.
ACP further recommends discussing screening discontinuation in asymptomatic women at average risk aged 75 years or older, or those with a limited life expectancy.
The guidance lastly recommends that for asymptomatic, average-risk women with breast density of Breast Imaging Reporting and Data System (BI-RADS) categories C or D, clinicians should:
- consider using supplemental digital breast tomosynthesis; and
- not use supplemental MRI or ultrasound.
Screening guidance varies across organizations
Crandall said the new guidelines are meant to reconcile conflicting recommendations across medical organizations.
The U.S. Preventive Services Task Force recommends biennial screening for women aged 40 to 74 years. The recommendation does not apply to women with a personal history of breast cancer, those who had a lesion on previous biopsies, and those who have a very high risk for breast cancer because of a history of high-dose radiation therapy to their chest at a young age or certain genetic markers. The task force said there was not enough evidence to make a recommendation for or against screening in women aged 75 years or older.
Meanwhile, the American College of Radiology (ACR) recommends annual breast cancer screening starting at age 40 years. It also recommends that all women receive a breast cancer risk assessment by age 25 years to determine if screening is needed earlier. Black and Ashkenazi Jewish women were specifically highlighted by ACR as those who may benefit from earlier screening, as research shows they are at much higher risk for breast cancer mortality compared with other populations.
The American Cancer Society (ACS) recommends that women have the option to begin screening at age 40 years, but by age 45 years, the society recommends annual screening. Also, beginning at age 55 years, women should have the option to switch to biennial screening or continue yearly mammograms.
Neither the ACS nor ACR recommendations were included in ACP’s assessment during the development of its guidelines because they “did not meet our inclusion criteria,” Crandall told Healio.
“Any guideline that is older than 5 years is considered expired since the data utilized is quite old. The ACS has not updated its breast cancer screening guideline since 2015,” she said. “ACP’s guidance statements focus on recently updated or published guidelines (last 5 years) because ACP aims to assess the most up-to-date evidence and clinical thinking to make guidance as useful as possible to clinicians and patients.”
ACR’s guidance, she noted, does not fit the definition of a clinical guideline because it was not based on a systematic review.
“The accepted definition of a guideline by National Academy of Medicine (NAM) and Guidelines International Network (GIN) clearly states that a document to be considered a guideline should have been informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options,” she said. “In addition, some organizations do not follow the currently acceptable standards to develop high-quality guidelines that have been recommended by NAM and GIN. Variation in methods, including following different processes for important and critical issues such as disclosure of interests and how conflicts of interest are managed … need to be kept in mind.”
Clashing views
Crandall said the ACP guidelines reflect the potential risks of more frequent mammography, including the possibility of more false positives, biopsies, radiation exposure, patient burden and costs.
“We’re trying to get the right balance,” she said during the plenary. “We have to feel comfortable with our best evidence out there.”
One notable difference between ACP and ACS guidelines is that the latter “didn’t specifically review whether breast cancer mortality is different with annual vs. biennial,” Crandall said. “But we really need more data regarding breast frequency.”
However, Robert A. Smith, PhD, senior vice president of early cancer detection science at ACS, said that ACP is “kind of behind the evolution of breast cancer screening” in some aspects.
“We understand that breast cancer screening is beneficial in women ages 40 to 49 years, so I think it’s not really necessary to position this for shared decision-making,” he told Healio. “In fact, having done that, they cast doubt on the value of breast cancer screening.”
Smith said that clinicians understand shared decision-making “as being something that you do to discuss prostate cancer screening, for example — it’s judged to be not clear that the possibility of harms against the possibility of benefits is a clear choice, and so it’s referred to as a highly preferent decision.”
“Informed decision-making simply means patients need to know why this test is beneficial and what to expect from it, and they certainly can choose not to undergo the test if they prefer,” he said. “But most women already, and for decades, have embraced mammography screening beginning at the age of 40 years.”
Smith additionally pointed out that asymptomatic, average-risk women with breast density of BI-RADS categories C or D “need supplemental imaging, and that can be done with ultrasound or MRI.”
“To not recommend that is essentially saying, ‘You should accept an incomplete examination,’” Smith said. “If you have areas of density in your breast where a radiologist is not able to say with confidence that there’s a tumor there or not, these other technologies — mainly MRI because its functional imaging, not anatomical imaging — penetrate that density.”
Smith said that ACS’ guidance is “quite useful, but doctors are very sensitive to what’s covered under the Affordable Care Act, and right now, the Affordable Care Act is under law that coverage has to exist according to an A or B rating from the [USPSTF].”
“I share everyone’s frustration when guidelines are different,” he said. “Guideline-developing organizations commonly do not collaborate.”
Ultimately, ACP’s guidance “is very conservative,” including when it comes to women aged 75 years and older, Smith said.
A recent study supports continued mammography in older women. The retrospective analysis found that women who were diagnosed with breast cancer at age 80 years or older had a 55% lower risk for recurrence and more than 70% lower risk for death if they were screened within 2 years of diagnosis.
Crandall stressed that the new ACP guidelines do not recommend discontinuing screening after 74 years.
“What we are saying, though, is to discuss discontinuation based on shared-decision making,” she said. “Thus far, we have few data from randomized trials among people aged beyond 74 years. But those data have not yet shown a decrease in mortality from breast cancer if you continue screening beyond age 74. There is evidence of harm from continuing screening — more tests, overdiagnosis and over treatment of something that would not necessarily cause symptoms or affect a person’s lifespan. That’s based on modeling studies. We really do need more data in this group.”
For more information:
Carolyn J. Crandall, MD, MS, MACP, and Robert A. Smith, PhD, can be reached at primarycare@healio.com.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<









Leave a Reply