February 02, 2026
2 min read
Key takeaways:
- Of commercially insured patients in 2024, 57.5% had one chronic condition, 11.5% had two and 9.1% had three.
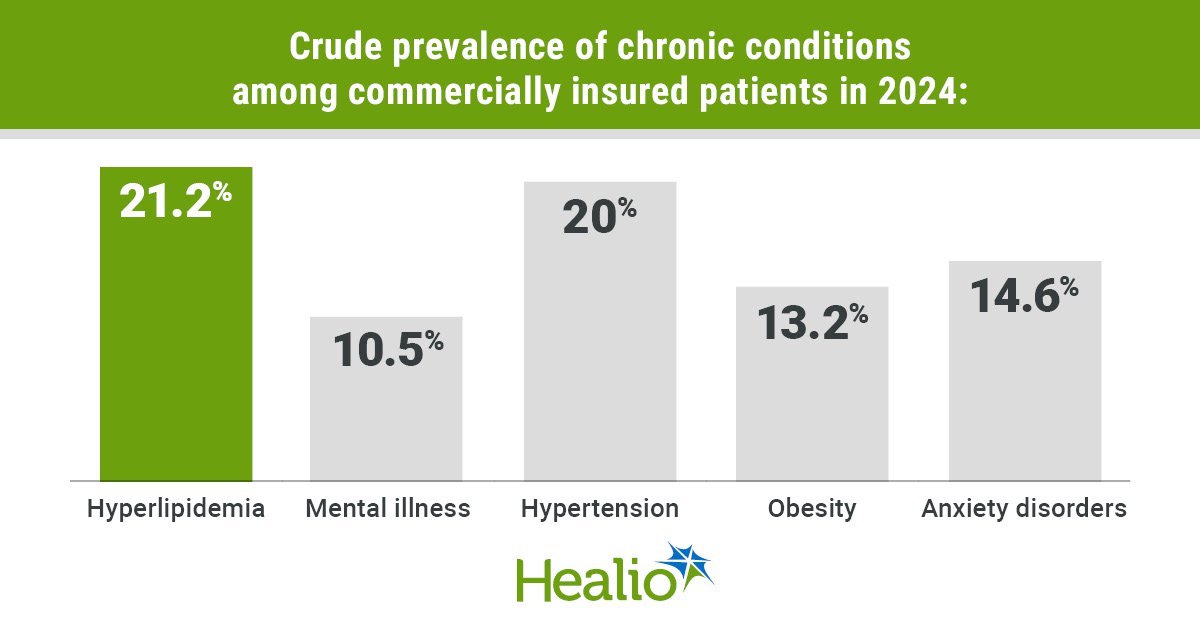
- Hyperlipidemia was the most common chronic condition.
Almost six in 10 commercially insured patients in the United States had at least one chronic condition in 2024, according to a new report from FAIR Health.
The findings follow other new data showing heart disease continues to be the leading cause of death in the country, underlining the need for greater chronic disease prevention.

Data derived from: Chronic conditions in the United States: A study of commercial claims.
The data “reinforce what many clinicians observe: chronic disease is now the norm rather than the exception,” Lenny Powell, DO, an osteopathic physician specializing in geriatrics and gerontology, and an associate professor of medicine at Rowan-Virtua School of Osteopathic Medicine, told Healio. “The fact that more than half of patients have at least one chronic condition, and many have multiple, underscores how dramatically the burden of disease has shifted over the past decade.”
Powell, who was not involved with the report, added the rise in health care costs tied to chronic conditions “is not surprising, but the magnitude is certainly striking.”
The report from FAIR Health — a nonprofit organization that provides information on health care coverage and insurance — captured the prevalence of 44 chronic conditions and their costs based on commercial claims in 2024.
FAIR Health’s researchers found that over half (57.5%) of commercially insured patients had at least one chronic condition in 2024, though many reported having two (11.5%) or three (9.1%) conditions.
Hyperlipidemia was the most common of all the chronic conditions assessed, with a crude prevalence of 21.2%, followed by hypertension (20%), anxiety disorders (14.6%), obesity (13.2%) and mental illness (10.5%).
Many conditions were co-occurring. Specifically, 33.4% of patients had obesity, hypertension, hyperlipidemia or some combination of these conditions, while 4.3% had all three, and half with one of the diseases had more than one.
When FAIR Health analyzed conditions in pairs, the crude prevalence of hypertension, hyperlipidemia, diabetes and obesity had a moderate to strong positive correlation.
The strongest positive correlation was seen for diabetes and hypertension (86%), while the weakest was for obesity and hyperlipidemia (45%).
Some conditions had more co-occurring comorbidities than others. Non-Alzheimer’s dementia, Alzheimer’s disease and acute myocardial infarction had the highest median number of comorbidities at six, while autism and pneumonia had the lowest at one.
FAIR Health’s report also indicated the number of chronic conditions a patient had greatly influenced the cost of health care. For example, the average allowed amount (the maximum amount that insurers will pay for a service before deductibles or coinsurance) for a patient with one chronic condition was $3,039 — almost twice as much as that of a patient with no chronic conditions ($1,590). The amount for a patient with 10 or more chronic conditions was $21,730 — 13.7 times higher vs. a person with no chronic diseases.
Prices additionally varied by condition. Of the 44 chronic conditions, lung cancer had the highest average allowed amount yearly ($22,740), while ADHD had the lowest ($4,175).
The poverty rate moderately positively correlated (53.5%) with the crude prevalence of hypertension. Some clusters of chronic conditions (specifically, the cluster of obesity, hypertension, diabetes, chronic kidney disease and hyperlipidemia) also strongly correlated with the poverty rate.
But all cancers weakly correlated with the poverty rate, with breast cancer having a correlation of –24.3%.
“Poverty remains a powerful driver of disease burden,” Powell said. “This reinforces the need for clinicians to screen for social determinants of health, and advocate for systems that support prevention, access and continuity of care.”
He also underlined that payment and care models “must continue to evolve to better support patients with multiple chronic conditions.”
FAIR Health noted their observational analysis had some limitations. The report was not peer-reviewed, and it excluded Medicare Advantage and Medicare Parts A, B and D beneficiaries.
Still, the findings “have implications for stakeholders across the health care spectrum, including patients, providers, payors, policymakers and researchers,” FAIR Health said.
According to Powell, multi-morbidity “should be considered the default framework for patient care.”
“Clinicians need to anticipate overlapping conditions, particularly metabolic clusters such as hyperlipidemia, hypertension, obesity and diabetes,” he told Healio. “They must manage them in an integrated way rather than in isolation.”
Powell concluded that prevention, “whether that is preventing the disease entirely or in a secondary manner, which prevents further complications and advancement with pharmacologic and other treatments … remains paramount.”
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<





Leave a Reply