January 29, 2026
5 min watch
Key takeaways:
- Lung cancer screening guidelines may exclude more than 60% of patients who develop the disease.
- Age-based screening could save more than 25,000 additional lives per year.
Current U.S. Preventive Services Task Force screening guidelines could exclude more than 60% of patients who develop lung cancer.
Conversely, an age-based approach to screening could save more than 25,000 lives per year.

Data derived from Yang HC, et al. JAMA Netw Open. 2025;doi:10.1001/jamanetworkopen.2025.46222.

Ankit Bharat
Ankit Bharat, MD, director of the Canning Thoracic Institute and Harold L. and Margaret N. Method Professor of Surgery at Northwestern University Feinberg School of Medicine, described current guidelines as “outdated and ineffective” with an overreliance on smoking history.
“We must urgently think about making lung cancer screening age-based and offer it to everybody in this country,” he told Healio.
Survival remains poor
Lung cancer is projected to cause 124,990 deaths in the U.S. in 2026, according to American Cancer Society’s (ACS) Cancer Statistics 2026 report. That is more than colorectal and pancreatic cancer — the next two deadliest malignancies — combined.
ACS reported 5-year survival rates for lung cancer have improved from 15% between 1995 and 1997 to 28% between 2015 and 2021. However, approximately 75% of patients are diagnosed with advanced-stage disease. Among those individuals, the 5-year survival rate is just 10%.
Current USPSTF screening guidelines recommend low-dose CT for adults aged 50 to 80 years who have at least a 20 pack-year smoking history, and who actively smoke or stopped within the previous 15 years, according to study background.
ACS noted 87% of lung cancer diagnoses in men and 84% in women could be attributed to smoking.
Bharat and colleagues have observed differently.
“In our day-to-day practice, we are seeing 30% to even 40% of all lung cancers are being diagnosed in people who may have had secondhand exposure, or who have never smoked,” Bharat said.
These experiences led researchers to investigate whether current screening criteria effectively captured the population of patients with lung cancer.
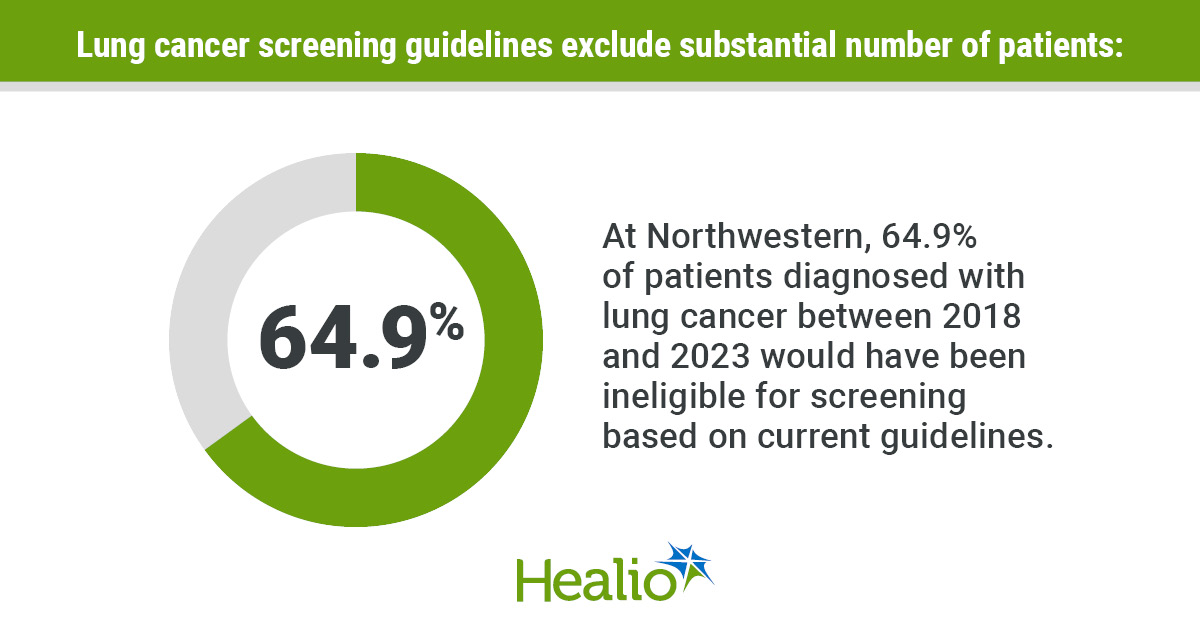
They included 997 consecutive individuals (58% women; 68% white) from Chicago metropolitan and surrounding areas diagnosed with lung cancer (median age at diagnosis, 67 years; range, 18-99) from September 2018 to March 20, 2023, at Northwestern.
Number of patients with lung cancer who met current screening criteria served as the primary endpoint. Survival, clinical characteristics and the impact expanded screening could have served as secondary endpoints.
‘Striking’ data
Overall, 64.9% of patients did not meet USPSTF screening criteria.
Among those, 38% never smoked and 57% either quit more than 15 years ago or had fewer than 20 pack-years of smoking history.
“We knew that a large percentage of patients were going to be ineligible, but the proportion was quite staggering for us,” Bharat said.
“Over a third of patients diagnosed with lung cancer were never-smokers. That was striking because these people often are young, the majority of them are women and they are at an age when they would be thinking of having a family or may have young kids.”
The group that did not meet screening criteria differed significantly from the group that did, and included younger patients (median age, 66 years vs. 69 years; P = .003), primarily women (61% vs. 52%; P = .004) and a greater proportion who identified as Asian (9.6% vs. 3.7%; P < .001).
Patients who did not meet screening criteria had significantly higher rates of adenocarcinoma (72% vs. 55%; P < .001) and significantly lower rates of small cell lung cancer (3.7% vs. 13%; P < .001) and squamous cell carcinoma (11% vs. 21%; P < .001).
They also had a significantly higher rate of stage I diagnoses (28% vs. 21%; P = .02) and lower rate of stage III cases (17% vs. 24%; P = .02). Both screening and non-screening eligible patients had similar rates of stage IV disease.
“Stage I lung cancer is completely curable; stage IV is not,” Bharat said. “Because people are generally not suspecting lung cancer, by the time they’re diagnosed, it’s much later stage.”
The entire cohort had a median OS of 6.56 years and 5-year survival rate of 54.6%.
Patients who never smoked had lower risk for death (HR = 0.49; 95% CI, 0.35-0.67).
Among smokers, mortality risk significantly declined if patients quit 10 to 30 years before diagnosis (HR = 0.73; 95% CI, 0.54-0.99) or at least 30 years before (HR = 0.65; 95% CI, 0.46-0.92).
The cohort that did not meet screening criteria had improved survival with treatment (HR = 0.67; 95% CI, 0.55-0.82).
They had significantly better median OS (9.5 years vs. 4.4 years) and 5-year (59.3% vs. 46.1%), 10-year (48.9% vs. 25.6%) and 15-year OS (36.1% vs. 20.3%).
Researchers observed worse survival for men (HR = 1.57; 95% CI, 1.29-1.91) and those with advanced disease (stage II: HR = 2.06; 95% CI, 1.32-3.22; stage III: HR = 2.88; 95% CI, 1.99-4.18; stage IV: HR = 5.97; 95% CI, 4.35-8.2).
Among patients who did not meet screening criteria, 24.8% would have been excluded for never smoking, 13% for quitting more than 15 years prior, 6.5% for not having 20 pack-years and 4.1% for not meeting age criteria.
A screening model that increased the age range (40-85 years), decreased pack-years (20 to 10) and removed the 15-year cessation limit would have captured 62.1% of the study population.
A screening model based on age alone (40-85 years) and not risk factors would have captured 93.9% of the study cohort.
Bharat and colleagues found 644 patients would need to receive a low-dose CT to prevent one lung cancer death. Comparatively, 3,037 patients need a breast cancer screen to prevent one death and 766 need a colorectal cancer evaluation.
If an age-based model detected 30% of stage I lung cancer diagnoses, researchers calculated 26,124 additional lives could be saved, more than breast and colorectal cancer combined (24,310).
The cost of each life saved from lung cancer would be $101,000, drastically lower than for breast cancer ($890,000) and colorectal cancer ($920,000).
“A low-dose CT scan, is relatively inexpensive generally costing less than a few hundred dollars,” Bharat said. “If you do a mammogram screening, which is an annual thing, depending on where it is done, it could be $2,000 to $3,000. Similarly, colonoscopies could be upwards of $5,000 per, and it requires people to get a bowel prep, go through anesthesia, all of that.
“Low-dose CT literally takes a few minutes to do, doesn’t require any contrast, and it gives information, not just about lung cancer, but also about your heart. We pick up other types of tumors. We pick up things like osteoporosis because you’re seeing spine and bone.”
Researchers acknowledged study limitations, including its single-institution design.
‘Very clear’
Future research into other risk factors for lung cancer remains pivotal, especially considering the high number of patients who never smoked.
Investigations into air pollution, radon, secondhand smoke, vaping, food, makeup and hairsprays are all warranted, Bharat said.
However, waiting for those findings could take years, if not decades.
“By that time, it’s too late. Thousands of lives are lost,” Bharat said. “Then what happens is many new things are added in our lives that could cause the same problem. We cannot keep chasing what’s causing the problem.”
The current data are “very clear,” he added. Universal age-based screening should be part of guidelines.
Northwestern Medicine is attempting to aid that cause. Any adult can get a low-dose CT to screen for lung cancer, and if their insurance does not pay for it, Northwestern will cover the cost as part of a clinical study.
Additionally, Bharat and colleagues are investigating if combining AI with low-dose CT could lead to detection of breast cancer, cardiovascular complications and other diseases so patients could pay one low cost to get all that information.
“We are trying to help the nation and other the medical communities make a jump,” Bharat said. “We are hoping that down the road, policymakers will look more favorably at making low-dose CT universally available.”
For more information:
Ankit Bharat, MD, can be reached at ankit.bharat@nm.org.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<





Leave a Reply