Key takeaways:
- Hypertensive disorders of pregnancy accounted for one-third of severe maternal morbidity from 2018 to 2022.
- The data show the importance of addressing cardiometabolic health before, during and after pregnancy.
WASHINGTON — Hypertensive disorders of pregnancy are the greatest drivers of rising severe maternal morbidity in the U.S., according to data presented at the ACOG Annual Clinical & Scientific Meeting.
Severe maternal morbidity, or SMM, “has been rising for years, and we kept describing the trend without explaining it,” Tetsuya Kawakita, MD, MS, an associate professor of obstetrics and gynecology at Eastern Virginia Medical School at Old Dominion University, told Healio. “We knew advanced maternal age, obesity and hypertensive disorders were all increasing, but no one had quantified how much of the rise each was actually driving. Without that, it’s hard to know where to focus prevention.”

Data derived from Jones S, Kawakita T. Decomposing 2018-2022 trends in severe maternal morbidity (excluding transfusion): Roles of hypertensive disorders of pregnancy, obesity, chronic hypertension, and pregestational diabetes mellitus. Presented at: ACOG Annual Clinical & Scientific Meeting; May 1-3, 2026; Washington.
In the retrospective analysis, Kawakita and Sora Jones, a medical student at Internal University of Health and Welfare in Japan, evaluated the delivery hospitalizations of 9,541,698 patients aged 11 to 55 years using 2018 to 2022 data from the Nationwide Readmissions Database.
They defined SMM using the CDC’s 21-indicator algorithm and adjusted for demographics and clinical covariates with multivariable logistic regression.
The researchers found that SMM prevalence rose from 0.78% to 0.91% from 2018 to 2022 (P < .001).
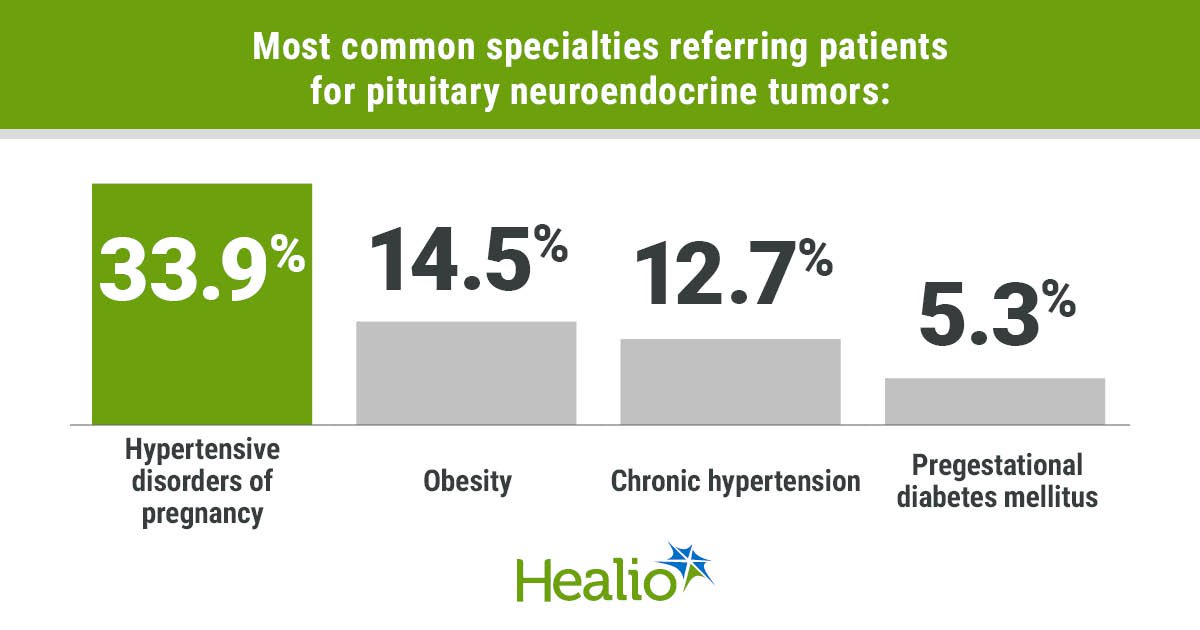
Hypertensive disorders of pregnancy were the largest contributors (33.9%), followed by obesity (14.5%), chronic hypertension (12.7%) and pregestational diabetes mellitus (5.3%), according to the abstract.
“The most striking finding was that hypertensive disorders of pregnancy alone explained roughly one-third of the rise in SMM, and more than half once we excluded transfusion,” Kawakita said. “A single category of conditions accounted for that much of a national trend.”
Kawakita and Jones reported that prior cesarean delivery, advanced maternal age and multiple gestation each contributed to under 5% of the rise.
Kawakita acknowledged it was surprising “how small a role advanced maternal age played. Maternal age gets a lot of public attention, but the real story here is cardiometabolic: hypertension, chronic hypertension and obesity. Even after accounting for all six risk factors, a meaningful portion of the increase remained unexplained, which is a reminder that social determinants and structural inequities are also part of this picture.”
According to Kawakita, consideration of cardiometabolic health before, during and after pregnancy is where prevention will have the most impact.
“Preconception counseling has to take BP, weight and glucose seriously. During pregnancy, we should be aggressive with low-dose aspirin for preeclampsia prevention and tighter BP control in chronic hypertension,” he told Healio. “Postpartum follow-up needs to be treated as a cardiovascular opportunity rather than an afterthought. Severe maternal morbidity is a cardiometabolic problem that happens to manifest during pregnancy, and care has to extend across the reproductive life course.”
Kawakita said the need moving forward is to determine if certain strategies, “such as preeclampsia prevention programs, chronic disease management and postpartum cardiovascular follow-up, actually move the population numbers. Given how much hypertensive disorders contributed, optimizing their care is a priority: delivery timing, BP targets and eclampsia prevention. The unexplained residual increase also points toward research on social determinants, maternity care deserts and structural racism.”
Ultimately, SMM trends “are not inevitable,” Kawakita said. “Hypertension, obesity and diabetes are conditions where prevention works. The rise in severe maternal morbidity reflects the broader cardiometabolic health of reproductive-age people in this country, and improving that upstream will improve maternal outcomes downstream.”
For more information:
Tetsuya Kawakita, MD, can be reached at primarycare@healio.com.
Sources/Disclosures
Source:
Jones S, Kawakita T. Decomposing 2018-2022 trends in severe maternal morbidity (excluding transfusion): Roles of hypertensive disorders of pregnancy, obesity, chronic hypertension, and pregestational diabetes mellitus. Presented at: ACOG Annual Clinical & Scientific Meeting; May 1-3, 2026; Washington.
Disclosures:
Kawakita and Jones report no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<











Leave a Reply