January 29, 2026
3 min read
Key takeaways:
- Those who used antidepressants had a lower likelihood of acute neurosurgical operations vs. those who did not.
- The mortality rate was 7.6% for those on antidepressants and 7.5% for those who were not.
Antidepressant use prior to traumatic brain injury was not associated with worse short-term outcomes for individuals including mortality, neurosurgical intervention or length of hospital stay, according to data published in Neurology.
“Concern remains that serotonergic antidepressants may worsen outcomes after traumatic brain injury (TBI) by increasing the risk of intracranial bleeding, yet high-quality population-level evidence on this issue has been lacking,” Jussi Posti, MD, PhD, associate professor of neurosurgery at the University of Turku in Finland, told Healio.

Data were derived from Posti J, et al. Neurology. 2026;doi:10.1212/WNL.0000000000214602.
Posti and colleagues sought to address this gap in the body of knowledge by combing nationwide registry data to examine the association between pre-injury antidepressant use, serotonergic profiles and short-term TBI outcomes in a real-world, unselected cohort.
“It addresses a common clinical dilemma at the intersection of neurotrauma, psychiatry and geriatric medicine,” Posti said.
They also aimed to investigate the short-term mortality outcomes in TBI, acute neurosurgical operations (ANOs) and length of hospitalization for the selected population.
Their retrospective cohort study included 54,876 individuals admitted to hospital with TBI in Finland between January 2005 and December 2018. Among these were 7,845 individuals with a record of antidepressants purchased within 90 days of TBI (mean age, 64.7 years; 56% women) and 47,031 without such a record (mean age, 60.6 years; 41.4% women).
Pre-injury antidepressant use was identified from national prescription records using a daily pill counting method and subcategorized by serotonergic profile (weak, intermediate, strong).
The primary outcome was 30-day mortality, while secondary outcomes included ANOs and length of hospitalization.
Covariates for analysis included age, sex, comorbidities, vitamin K antagonist use, admission location and study year. Results were expressed in either hazard ratios or relative risk.
From the 7,845 individuals who were using antidepressants at the time of TBI, 1,113 were termed “intermediate” strength, 1,626 were termed “weak” and 5,106 termed “strong” based on serotonergic profile.

Jussi Posti
According to results, 4,105 patients died within the 30-day mortality window, with the mortality rate being 7.6% for those with antidepressants and 7.5% for those without. Mortality rates among those with antidepressants were 10% in the weak group, 7.1% for the strong group and 6.3% for the intermediate group.
The researchers reported that adjusted models showed no significant association between antidepressant use and 30-day mortality (adjusted HR = 0.98; 95% CI: 0.9–1.07), nor were there significant associations between mortality and either serotonergic profile or type of antidepressant.
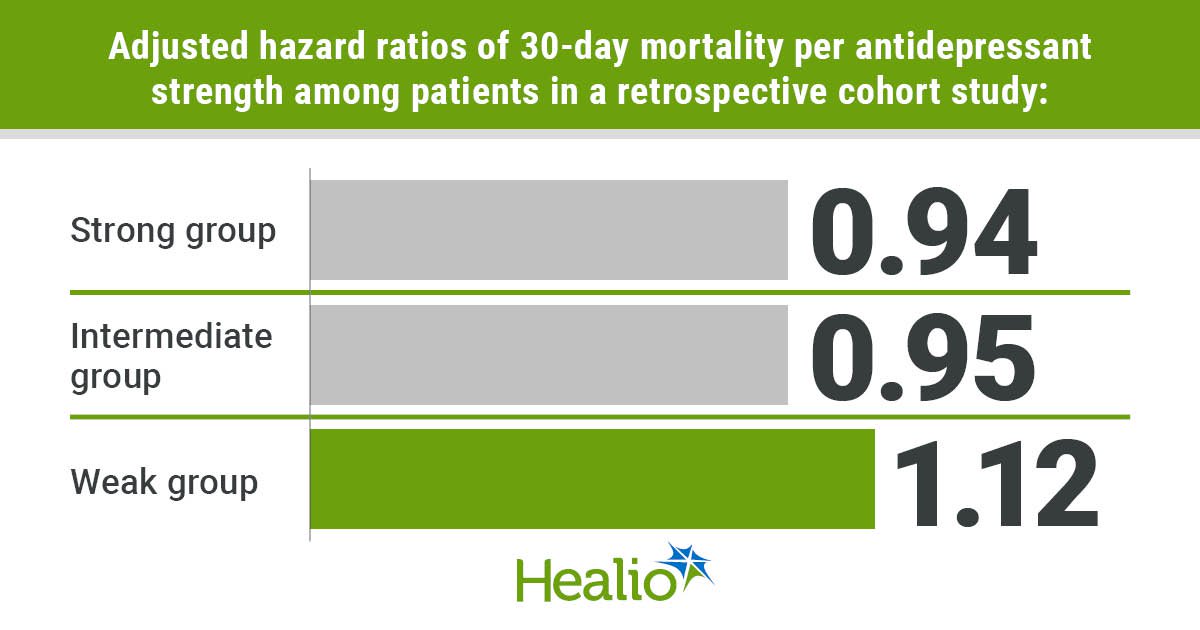
Compared with controls, the adjusted HRs of 30-day death for each antidepressant group were: 0.94 (95% CI: 0.84-1.05) for the strong group; 0.95 (95% CI: 0.75-1.2) for the intermediate group; and 1.12 (95% CI: 0.95-1.31) for the weak group.
However, Posti and colleagues noted that those who used antidepressants recorded a lower likelihood of ANOs (adjusted RR = 0.89; 95% CI: 0.82–0.97) compared with those who did not use antidepressants. ANO was performed for 4,586 patients with TBI, with mortality rates of 6.8% in the antidepressant users’ group and 8.6% in those without.
Patients who were using antidepressants had lower likelihood for ANO than patients not using them (aRR = 0.89; 95% CI: 0.82–0.97). The ANO rate was 6.5% in the strong group, 7.6% in the intermediate group and 7.2% in the weak serotonergic group.
Data additionally showed that serotonergic classes of antidepressant were associated with likelihood of ANO. The RR of ANO was lower for the strong group vs. controls (aRR = 0.88; 95% CI: 0.79–0.97) but similar for intermediate (aRR 0.89; 95% CI: 0.73–1.09) and weak (aRR = 0.92; 95% CI: 0.78–1.09) serotonergic groups and controls.
Length of hospitalization did not differ between groups, while neither antidepressant use, profile, nor type modified the association of VKA use with increased mortality or ANOs, the researchers wrote.
“This provides clinically reassuring evidence that antidepressant therapy alone should not be considered a risk modifier in acute traumatic brain injury management,” Posti told Healio. “The results support evidence-based decision-making in the growing population of older patients with psychiatric comorbidity and elevated traumatic brain injury risk.”
For more information:
Jussi Posti, MD, PhD, can be reached at psychiatry@healio.com.
Sources/Disclosures
Source:
Posti J, et al. Neurology. 2026;doi:10.1212/WNL.0000000000214602.
Reference:
Antidepressants not associated with serious complications from TBI. https://www.aan.com/PressRoom/Home/PressRelease/5309. Published Jan. 28, 2026. Accessed Jan. 29, 2026.
Disclosures:
Posti reports receiving speaker’s fees from the Finnish Association of Otorhinolaryngology – Head and Neck Surgery, the Finnish Medical Association, Sanofi, Wellbeing services county of North Karelia; receiving travel expense reimbursement and expert fees from the National Institute of Neurological Disorders and Stroke; receiving support from the Research Council of Finland and the Sigrid Juselius Foundation. Please see the study for all other authors’ relevant financial disclosures. The study was funded by the Finnish Foundation for Cardiovascular Research, the Paavo Nurmi Foundation and the Paulo Foundation.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<











Leave a Reply