January 15, 2026
3 min read
Key takeaways:
- A similar proportion of patients in the high and low PEEP groups experienced pulmonary complications after surgery.
- More patients receiving higher vs. lower PEEP experienced intraoperative complications.
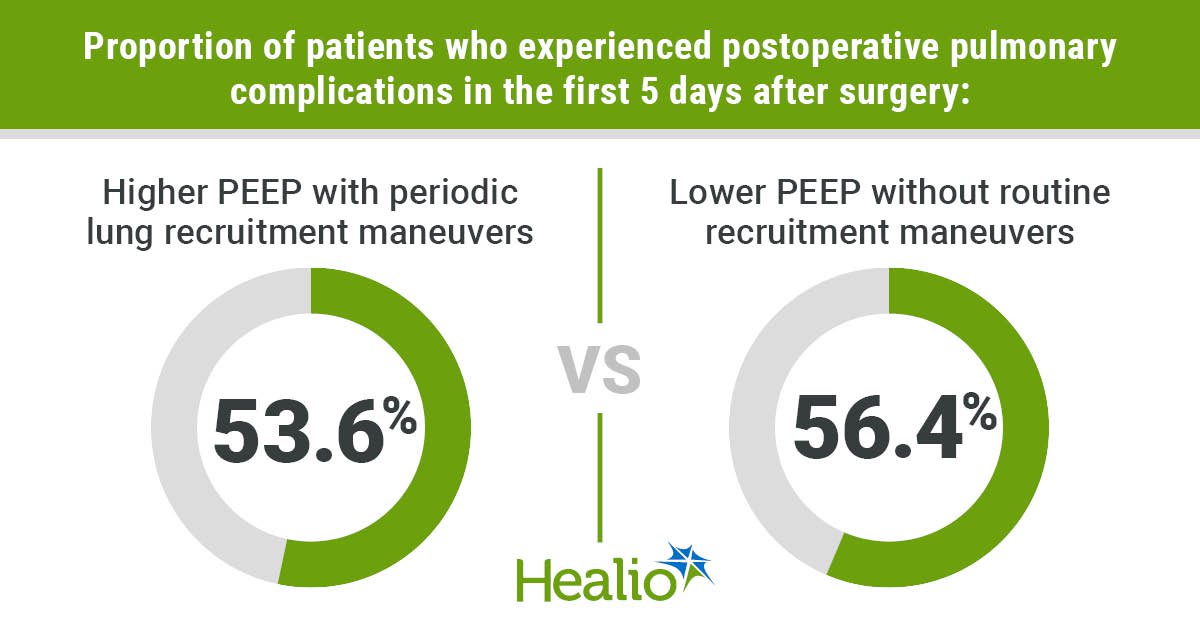
The proportion of patients with postoperative pulmonary complications in the first 5 days after thoracic surgery did not differ based on one-lung ventilation using higher or lower positive end-expiratory pressure, according to study data.
Higher PEEP was paired with periodic lung recruitment maneuvers, whereas lower PEEP was paired with no routine recruitment maneuvers, according to results published in The Lancet Respiratory Medicine.

Data were derived from Writing Committee, et al. Lancet Respir Med. 2025;doi:10.1016/S2213-2600(25)00330-3.
“For everyday clinicians, our findings suggest that routine use of higher positive end-expiratory pressure (PEEP) with recruitment maneuvers during one-lung ventilation should be reconsidered, and that ventilatory strategies should be individualized based on each patient’s gas exchange and hemodynamic status to optimize safety and outcomes,” Jakob Wittenstein, MD, clinician scientist and fellow at University Hospital Carl Gustav Carus Dresden, told Healio.
In the multicenter, international, randomized, controlled phase 3 PROTHOR study, researchers evaluated 2,124 adults who underwent open thoracic or video-assisted thoracoscopic surgery under general anesthesia requiring one-lung ventilation with a double-lumen tube to uncover if the number of patients with pulmonary complications reported in the first 5 days after surgery differs based on use of higher PEEP (10 cm H2O) and periodic lung recruitment maneuvers vs. lower PEEP (5 cm H2O) without routine recruitment maneuvers.
Included patients also had a BMI less than 35 kg/m2, a planned operative time of longer than 60 minutes and an expected one-lung ventilation duration longer than that of two-lung ventilation, according to the study.
“The study was prompted by ongoing uncertainty about whether higher PEEP with recruitment maneuvers during one-lung ventilation in thoracic surgery actually reduces postoperative pulmonary complications, as previous evidence was inconclusive and clinical practice varied widely,” Wittenstein said.
In both groups, researchers wrote that protective tidal volumes were given during one-lung ventilation (5 mL/kg predicted body weight) and two-lung ventilation (7 mL/kg predicted body weight).
Notably, 14 postoperative pulmonary complications made up the composite outcome: aspiration pneumonia, moderate respiratory failure, severe respiratory failure, acute respiratory distress syndrome, pulmonary infection, atelectasis, cardiopulmonary edema, pleural effusion, nonoperative pneumothorax, pulmonary infiltrates, prolonged air leak, purulent pleuritis, pulmonary embolism and pulmonary hemorrhage.
The high PEEP group included 1,056 patients (median age, 63.5 years; 58% men; median BMI, 25.6 kg/m2), and the low PEEP group included 1,068 patients (median age, 63 years; 57.4% men; median BMI, 25.5 kg/m2).
When evaluating ventilation and intraoperative characteristics between the two groups, the study outlined that the high vs. low PEEP group had higher peak pressure, higher plateau pressure, lower driving pressure, higher SpO2 during one-lung ventilation and at the end of surgery, and a longer duration of anesthesia.
Researchers found a similar proportion of patients who experienced postoperative pulmonary complications in the first 5 days after surgery in the high PEEP group and the low PEEP group (53.6% vs. 56.4%; absolute risk difference, –2.68 percentage points; 95% CI, –6.36 to 1.01). This was also the case when assessing extrapulmonary postoperative complications in the high and low PEEP groups (10.6% vs. 10.2%).
Switching to intraoperative complications, a greater proportion of patients receiving the higher vs. lower PEEP experienced this type of complication (49.8% vs. 31.3%; absolute risk difference, 18.09 percentage points; 95% CI, 14.41-21.77).
The study specifically highlighted that more patients receiving higher vs. lower PEEP experienced hypotension (37.3% vs. 14.3%) and new arrhythmias (9.9% vs. 3.9%). In contrast, more patients receiving lower vs. higher PEEP had hypoxemia that required rescue maneuvers (8.8% vs. 3.3%).
“It was somewhat surprising that higher PEEP with recruitment maneuvers did not reduce postoperative pulmonary complications and, in fact, led to more intraoperative complications such as hypotension and arrhythmias, contrary to what some earlier studies in one-lung ventilation had suggested,” Wittenstein told Healio.
Lastly, patients in the high PEEP group had a total of 209 adverse events, which was comparable to the 204 adverse events in the low PEEP group.
“Future studies will likely focus on perioperative strategies that extend beyond the intraoperative period,” Wittenstein said.
For more information:
Jakob Wittenstein, MD, can be reached at jakob.wittenstein@ukdd.de.
Sources/Disclosures
Source:
Writing Committee, et al. Lancet Respir Med. 2025;doi:10.1016/S2213-2600(25)00330-3.
Reference:
Disclosures:
One author reports receiving consulting fees from Ambu for participation in a data and safety monitoring board. Another author reports working part-time as research coordinator at Hamilton Medical (Bonaduz, Switzerland), unrelated to the current study. All other authors report no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<











Leave a Reply