April 30, 2026
2 min read
Key takeaways:
- Renin-angiotensin-aldosterone system (RAAS) inhibitors conferred reduced risks for starting dialysis or needing a kidney transplant.
- Risks for any adverse event were lower in the RAAS inhibitor treatment group.
Renin-angiotensin-aldosterone system inhibitors were linked to better pediatric chronic kidney disease outcomes compared with calcium channel blockers, according to study data published in JAMA Pediatrics.
Renin-angiotensin-aldosterone system (RAAS) inhibitors and calcium channel blockers (CCBs) are two primary antihypertensive treatments used in the pediatric population, according to Michelle R. Denburg, MD, MSCE, associate professor of pediatrics (nephrology) at the Children’s Hospital of Philadelphia, and colleagues. However, few trials have compared the effectiveness of both antihypertensive medications in a cohort of pediatric patients with CKD, they wrote.

Data derived from Denburg MR, et al. JAMA Pediatr. 2026;doi:10.1001/jamapediatrics.2026.0207.
“We used target trial emulation methods to evaluate the real-world comparative effectiveness of the most widely used first-line antihypertensive treatments in pediatric CKD,” Denburg and colleagues wrote.
In a comparative effectiveness study, the researchers reviewed electronic health record data from 1,757 children and adolescents prescribed RAAS inhibitors (median age, 13.1 years; 51.1% boys; 46.9% white) and 1,005 prescribed CCBs (median age, 12.6 years; 50.2% girls; 45.5% white) from the PRESERVE study from 2009 to 2020. Patients were included if they had CKD stage 2 to 4 and a systolic blood pressure higher than the 90th percentile or a hypertension diagnosis.
The primary outcome evaluated whether patients began a kidney replacement therapy treatment (dialysis or kidney transplant) within 2 years. The secondary outcome was a composite of starting a kidney replacement therapy, eGFR decline of at least 50% or kidney failure.
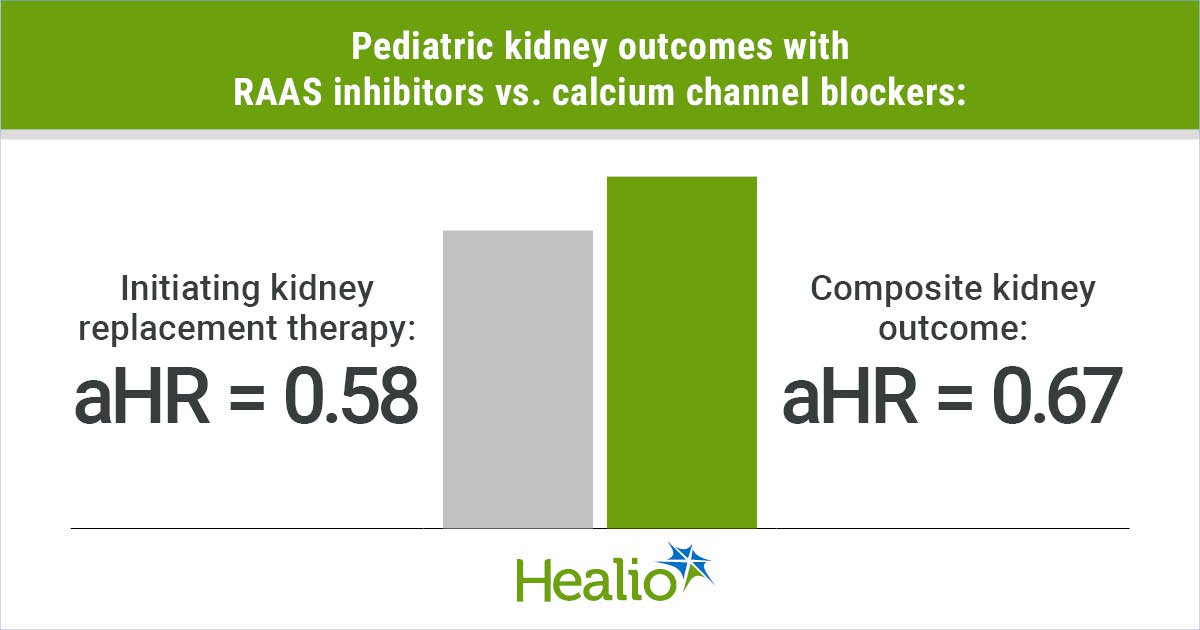
Results showed patients treated with RAAS inhibitors had reduced risks for initiating kidney replacement therapy (adjusted HR = 0.58; 95% CI, 0.4-0.84) and the composite outcome (aHR = 0.67; 95% CI, 0.53-0.83) compared with CCBs.
Additionally, patients treated with RAAS inhibitors had better systolic BP control compared with CCBs, defined by the amount of time spent above the 90th percentile for systolic BP (29% vs. 39%).
Compared with CCBs, RAAS inhibitors were associated with lower risks for any adverse event (HR = 0.82; 95% CI, 0.74-0.9), edema (HR = 0.76; 95% CI, 0.59-0.98), anemia (HR = 0.74; 95% CI, 0.62-0.89), leukocytopenia (HR = 0.76; 95% CI, 0.62-0.93), stomatitis (HR = 0.41; 95% CI, 0.26-0.67) and elevated liver enzymes (HR = 0.71; 95% CI, 0.54-0.92). Conversely, the RAAS inhibitor group had greater risks for hypotension (HR = 1.55; 95% CI, 1.03-2.35) and hair loss (HR = 1.94; 95% CI, 1.02-3.69).
Exploratory subgroup analysis showed patients with nonglomerular disease had significantly lower risks for beginning kidney replacement therapy (aHR = 0.53; 95% CI, 0.32-0.88) and the composite outcome (aHR = 0.62; 95% CI, 0.41-0.81). Changes among patients with glomerular disease did not reach statistical significance, according to the researchers.
Overall, RAAS inhibitor use was associated with better kidney preservation and BP control vs. CCBs, according to the researchers.
“These findings support first-line use of RAAS inhibitors for antihypertensive therapy in children with CKD,” Denburg and colleagues wrote.
Perspective
Back to Top

Darcy K. Weidemann, MD, MHS, FAAP
Disclosures: Weidemann reports no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<









Leave a Reply