April 13, 2026
2 min read
Key takeaways:
- Hydralazine did not increase vasculitis risk when accounting for the competing risk for death.
- Vasculitis risk “should probably not be the main factor” in considering hydralazine, the researchers wrote.
Hydralazine does not increase the risk for vasculitis in individuals using the medication for cardiovascular disease, according to findings published in JAMA Network Open.
“Reports of autoimmunogenic activity with hydralazine use first emerged in the 1980s with case reports of drug-induced lupus, cutaneous leukocytoclastic vasculitis and antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV),” Deena Fremont, MSc, of the Ottawa Hospital Research Institute, and colleagues wrote. “Hydralazine-associated vasculitis may present with pulmonary-renal syndrome, rapidly progressive glomerulonephritis, and permanent kidney or lung damage.

Data were derived from Fremont D, et al. JAMA Netw Open. 2026:doi:10.1001/jamanetworkopen.2026.1943.
“As such, the product monograph warns of autoimmune disease as a potential adverse event and recommends periodic routine monitoring for a complete blood cell count, antinuclear factors, and urinary abnormalities,” they added. “Clinical trials report only one case of lupus-like syndrome in more than 700 individuals randomized to hydralazine. Despite their inherent potential biases, health administrative databases are a useful method to examine rare adverse drug events. To date, the true extent of autoimmune-related adverse events, such as AAV, with hydralazine use remains uncertain.”
In a population-based, retrospective cohort study, Fremont and colleagues aimed to assess the risk for vasculitis associated with hydralazine vs. angiotensin-converting enzyme inhibitors (ACE) or angiotensin receptor blockers (ARB). Eligible participants were aged 66 years or older, and had been prescribed hydralazine for outpatient use between Jan. 1, 2008, and Dec. 31, 2021. A diagnosis of vasculitis served as the primary endpoint.
The overall study population included 583,136 adults from Ontario, Canada, with a mean age of 73 years (standard deviation, 7.2). The cohort was 55.2% women. A total of 40,748 participants had been prescribed hydralazine, while 542,388 patients were observed in the ACE or ARB group.
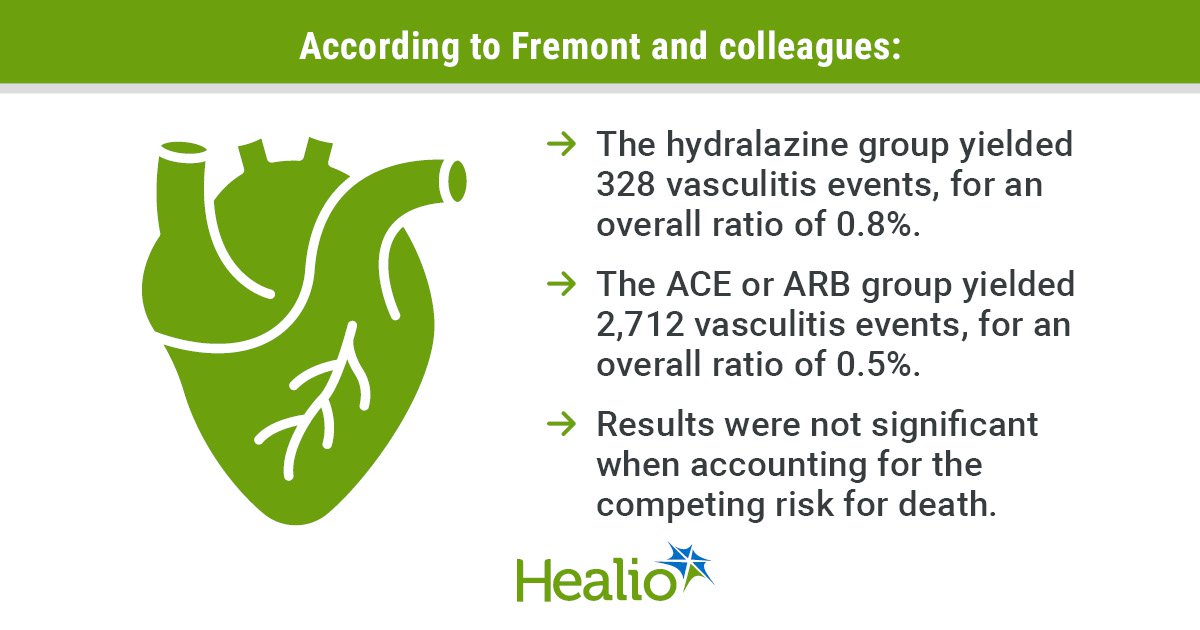
According to the findings, the hydralazine group yielded 328 vasculitis events for an overall ratio of 0.8%, which the researchers noted was higher than the 2,712 events (0.5%) in the ACE or ARB group (absolute risk difference, 0.3 percentage points; HR = 1.19; 95% CI, 1.04-1.37).
However, when the competing risk for death was factored into the analysis, the difference was no longer statistically significant.
“In this cohort study of adults who were newly prescribed hydralazine, the use of hydralazine may be associated with a small measurable risk of vasculitis compared with ACE or ARB use; however, this finding did not appear to represent a clinically meaningful risk given the rarity of the disease,” Fremont and colleagues wrote. “Although our findings did not determine whether hydralazine caused vasculitis, concern for vasculitis should probably not be the main factor driving a clinician’s decision on the appropriateness of using hydralazine for their patient.”
The hydralazine group yielded 328 vasculitis events, for an overall ratio of 0.8%.
The ACE or ARB group yielded 2,712 vasculitis events, for an overall ratio of 0.5%.
Results were not significant when accounting for the competing risk for death.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<








Leave a Reply