April 17, 2026
2 min read
Key takeaways:
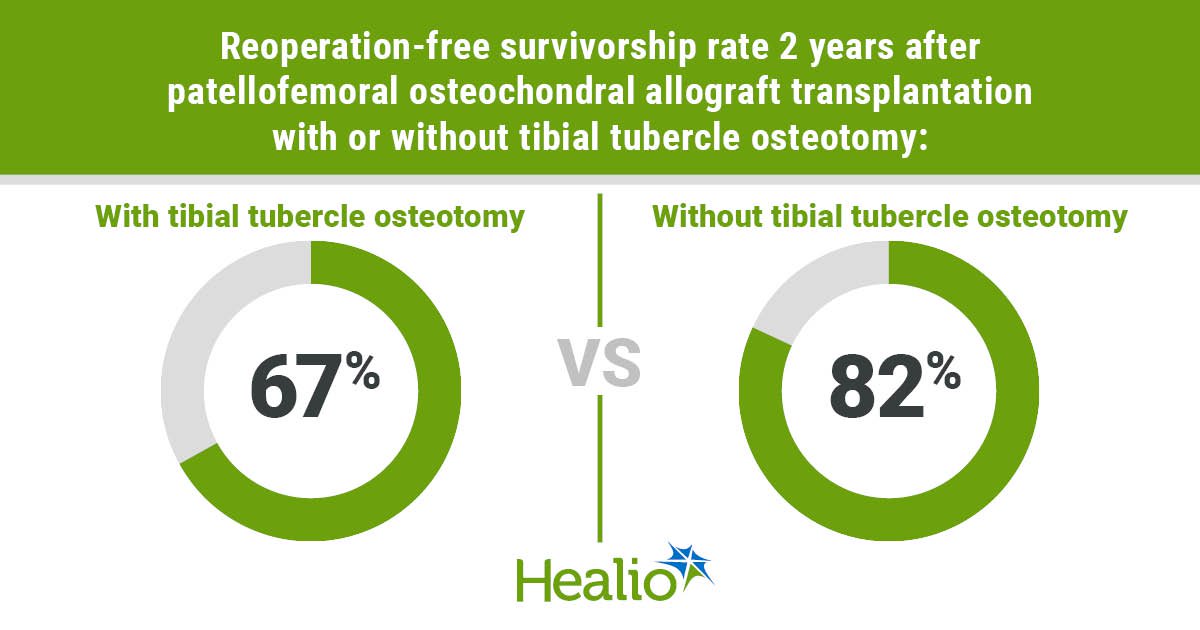
- Osteochondral allograft transplantation with osteotomy had a 67% reoperation-free survivorship.
- Graft diameter and multiple lesions increased the risk for reoperation with tibial tubercle osteotomy.
NEW ORLEANS — Concomitant tibial tubercle osteotomy did not improve graft survivorship among patients undergoing patellofemoral osteochondral allograft transplantation, according to results presented here.
“Typically, with cartilage grafts around the knee, the idea is that we want to unload the patella to take pressure off to allow the cartilage to heal,” Laith M. Jazrawi, MD, FAAOS, chief of sports medicine and director of the sports medicine fellowship at NYU Langone Health, told Healio about results presented at the American Academy of Orthopaedic Surgeons Annual Meeting. “What we found in our study when we used osteochondral allografts, which have bone and cartilage, is that the addition of a tibial tubercle osteotomy did not improve the outcomes in these patients and, many times, there were more complications associated with healing issues with the tibial tubercle osteotomy.”

Data derived from Sundaram V, et al. Paper 509. Presented at: American Academy of Orthopaedic Surgeons Annual Meeting; March 2-6, 2026; New Orleans.

Laith M. Jazrawi

Vishal Sundaram
Jazrawi, along with Vishal Sundaram and colleagues, retrospectively reviewed data from 103 patients who underwent patellofemoral osteochondral allograft transplantation with (n = 39) or without (n = 64) a tibial tubercle osteotomy (TTO) between 2001 and 2023. In his presentation, Sundaram said the primary outcome was graft failure, defined as progression to arthroplasty, revision cartilage surgery, subchondral collapse on imaging or failed graft incorporation on second-look arthroscopy, and secondary outcome was all-cause reoperation, defined as any subsequent ipsilateral knee surgery.
“We compared all these variables between our groups, including Kaplan-Meier survivorship to adjust for variable follow-up time,” Sundaram, fourth-year medical student at NYU Langone Health, said in his presentation. “We performed an identical subanalysis with propensity-matched groups.”
According to Sundaram, graft failure rates did not differ in patients who underwent patellofemoral osteochondral allograft transplantation with and without TTO, with a Kaplan-Meier survivorship of 95% at 2-year follow-up. However, patients who received TTO had a reoperation-free survivorship rate of 67% at 2 years compared with 82% in patients who did not receive TTO.
“This reoperation difference was, of course, largely driven by TTO-related hardware complications, as one may expect,” Sundaram said.
When patients were matched for sex, alignment parameters and lesion characteristics, Sundaram said there were no significant difference in graft failure or reoperation.
“To identify the factors that did predict reoperation or failure, we brought it back to our original unmatched cohort and, in the [osteochondral allograft] only group, we found a larger total graft diameter — specifically greater than 27.5 mm — was significantly predictive of graft failure,” Sundaram said.
Although graft diameter greater than 21 mm and the presence of multiple lesions were associated with increased risk for reoperation in the TTO group, Sundaram said graft size was not associated with graft failure.
“Surgeons should carefully weigh the risks of additional surgery when considering augmentation of a patellofemoral osteochondral allograft transplantation with a TTO for graft preservation,” Sundaram said.
For more information:
Laith M. Jazrawi, MD, FAAOS, and Vishal Sundaram wish to be contacted through Marlene Naanes at marlene.naanes@nyulangone.org.
Sources/Disclosures
Source:
Sundaram V, et al. Paper 509. Presented at: American Academy of Orthopaedic Surgeons Annual Meeting; March 2-6, 2026; New Orleans.
Disclosures:
Jazrawi and Sundaram report no relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data
<










Leave a Reply